1) Surgery can be defined as the art and science of treatment and is commonly grouped according to purpose, urgency, and risk level.
2) Pre-operative care involves assessing and preparing the patient physically and psychologically for surgery through education, consent, and correcting health issues.
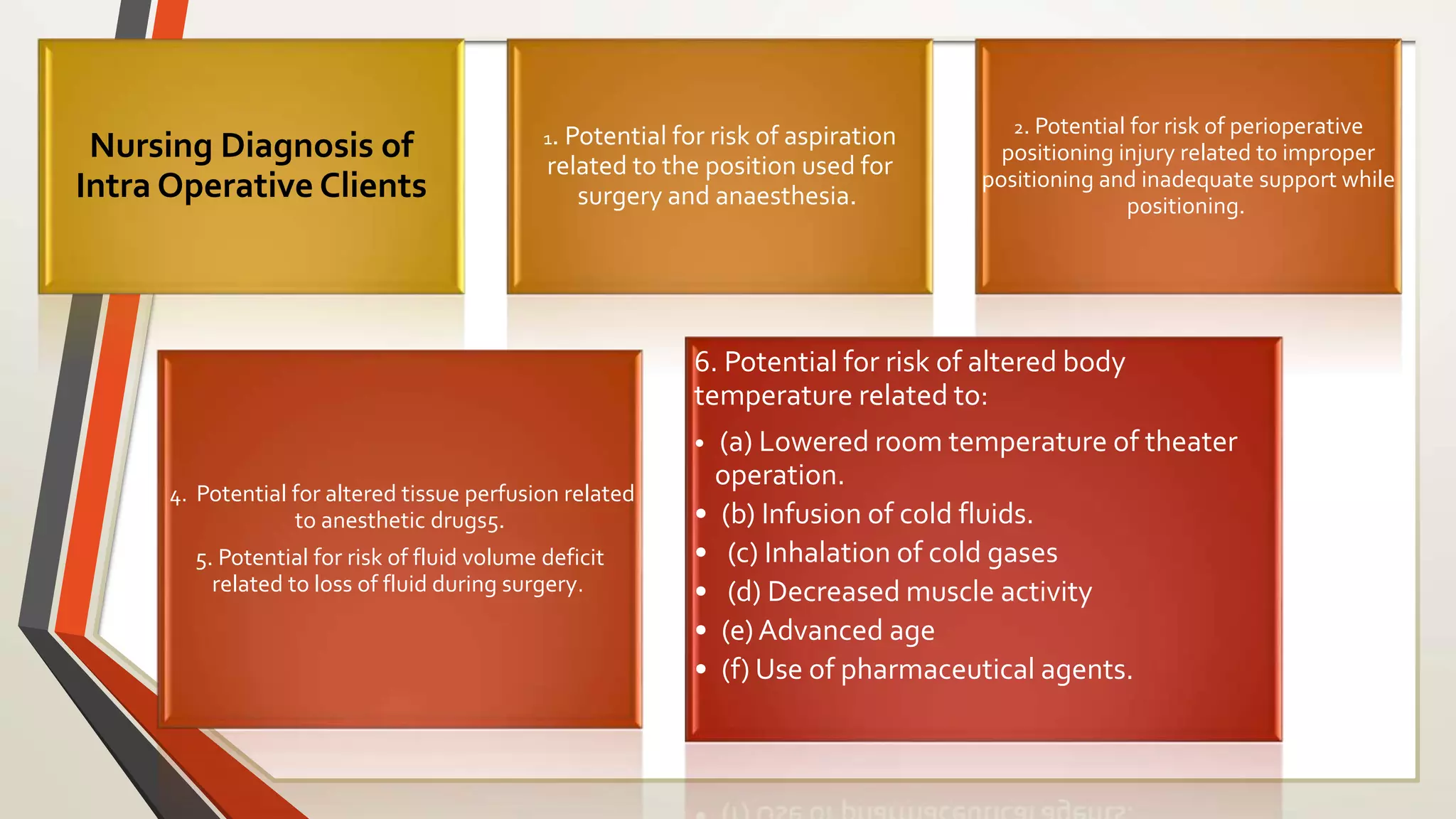
3) Intra-operative care is provided by anesthesiology, surgical, and operating room nursing teams to ensure patient safety and coordination during the procedure.






























































































![Review of literature [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reviewofliteratureautosaved-230315053854-fbe61789-thumbnail.jpg?width=640&height=640&fit=bounds)

![Bandages and Binders [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bandagesandbindersautosaved-230314063514-38348509-thumbnail.jpg?width=640&height=640&fit=bounds)



















