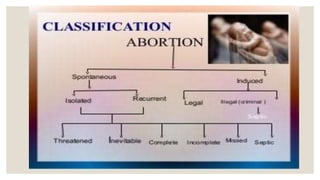
This document discusses high risk pregnancies and abnormal pregnancies. It covers various causes of bleeding in early pregnancy like miscarriage, ectopic pregnancy, molar pregnancy and their signs and symptoms. It also discusses disorders caused by or associated with pregnancy like preeclampsia. Other high risk conditions discussed include infections, cardiac/renal problems, fibroids and pelvic abnormalities. Types of miscarriages like threatened, inevitable, incomplete and septic abortions are explained along with their management. Recurrent miscarriages and investigations for their causes are also summarized.









































![ABORTION -POST ABORTIVE CARE[1][2] ner.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abortion-postabortivecare12ner-250903092827-23f6f291-thumbnail.jpg?width=640&height=640&fit=bounds)
























![Review of literature [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reviewofliteratureautosaved-230315053854-fbe61789-thumbnail.jpg?width=640&height=640&fit=bounds)

![Bandages and Binders [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/bandagesandbindersautosaved-230314063514-38348509-thumbnail.jpg?width=640&height=640&fit=bounds)


















