Acknowledgements
• Addisa AbabaUniversity
• Jimma University
• Hawassa University
• Haramaya University
• University of Gondar
• American Society for Clinical Pathology
• Center for Disease Control and Prevention-Ethiopia
2
3.
Chapter Objective
At theend of this chapter the students will be able to describe
Microscopic examination for urine sediment
Normal and abnormal organized urine sediments with their
diagnostic features.
Formation and significance of casts
Normal and abnormal crystals encounter in urine sediments
Relationship between sediments, chemical, physical findings in
urine
Reporting of urinary sediments
Quality control in urinalysis.
3
4.
Chapter Outline
Microscopic ExaminationOf Urine
Procedure for microscopic examination
Source of errors in the microscopic examination of urine
Urinary Sediments
Organized Urinary Sediments
Parasite, fungus and bacteria in urine
Non-Organized Urinary Sediments Urine Crystals
Body cells, crystals, casts, yeasts, bacteria, sperm
Methods of reporting formed elements
Quality control in urinalysis.
4
5.
Introduction
• In examiningurinary sediment it is necessary to learn the
distinguishing characteristics of elements which have clinical
significance .
• If the urine sample is properly collected, the test is carefully
performed, and the person performing the test is knowledgeable,
skillful valuable information can be obtained from microscopic
examination of urine specimen.
• Normally small amount of solid substances is found in the urine.
But when their concentration become high, may indicate the
existence of abnormal physiological function of our body.
5
6.
Standardization
• Aspects ofmicroscopic examination that
should be standardizes:
1. Volume of urine analyzed
2. Length and force of centrifugal
3. Re-suspending volume and concentration of sediment
4. Volume and amount of sediment examined
5. Terminology and reporting format
6
7.
Principles of method
Centrifuge10-12 ml urine specimen at 1500 – 2000 rpm for 3-5
minutes then discard the supernatant by quick inversion of the
tube, resuspend and take the sediment by Pasteur pipette from
the tube, transfer a drop into the clean and dry slide finaly
examin on the microscope
• Repeated evaluation of urine sediment is frequently valuable in
following the course and management of urinary tract disorders,
because the appearance of cellular elements, and casts in the
urine is a reflection of changes that take place in the kidney.
7
8.
Reagents and equipment
•Assemble all necessary materials used for the collection,
centrifugation and examination.
– centrifuge.
– Conical centrifuge tubes, or regular test tubes.
– Pasture pipette with rubber fit or automatic pipettes if
possible.
– Slides and cover slides 20 x 20 mm.
– Microscope
– Some staining reagents if needed (gram stain,10% KOH
and A crystal violet safranin stain ,etc)
– Specimen collecting cup
8
9.
Specimen requirement
• Preparationof patient
• Instruct the patient how to collect the specimen. The first morning
urine or mid-stream urine specimen is more preferable, because it is
more concentrated and formed elements are less likely disintegrated
• Explain the purpose of the test by using simple language. Do not use
medical terms or try to explain details of the procedure.
• If the patient is female, advice her to wash her genital organ before
giving the specimen. This is because bacteria that are normally found
on the genital tract may contaminate the sample and affect the result.
9
10.
Specimen requirement cont’d…
•Instruct the patient to collect at least 15 ml of urine in to the clean,
sterilize and dry urine cup that is supplied from the laboratory.
• The collected urine sample should arrive at a diagnostic laboratory as
soon as possible.
• If the urine sample is delayed by more than 2 hours, without
preservation, urine sediment appearance and constituent may be
changed and false results may be obtained and reported.
• If it is difficult to deliver within 2 hrs, it is better to preserve specimen
in the refrigerator at the temperature between 2-6 0C or use chemical
preservatives.
10
11.
Procedure for MicroscopicExamination
1. Mix the urine specimen
2. Transfer about 10 ml of urine into a labelled centrifuge tube.
3. Centrifuge the specimen at a medium speed (from 1500 – 2000 rpm)
for 3-5 minutes
4. Discard the supernatant by quick inversion of the tube
5. Re suspend the sediment that is at the bottom of the tube, by tapping
the tube by your fingers
6. Take the sediment by Pasteur pipette from the tube and transfer a drop
into the clean and dry slide.
11
12.
Procedure for Microscopic
Examination
•Apply cover slide on the urine sediment that is on the slide.
• Put on the microscope and look under 10x objective of the
microscope.
• Then after looking through the low power objective, change the
objective in to 40x objective .
• Then report what you get under low power and high power objective
on the laboratory request form of the patient.
12
13.
Source of Errors
•Drying of the specimen on the slide.
• If the supernatant fluid after centrifugation is not poured off
properly, it may decrease concentration of urine sediments and
false result may be reported
• If the whole sediment with supernatant is discarded during
inverting down the tube for long period, the whole sediments will
be discarded and so again false negative result will be reported.
• Thus another sample should be collected and the test repeated.
13
14.
Classification of UrinarySediments
• Urine sediments can grossly be categorized into
• organized and
• non-organized sediments
based on the substances they are composed of.
14
Organized Urinary Sediments
REDBLOOD CELLS
not usually present in normal urine.
• Appearance:
– Normally RBCs appear in the fresh sample as intact, small and
faint yellowish discs, darker at the edges
• Measure 7-8 m
• In concentrated urine may be crenated and became small (5-6 m)
• In diluted urine, RBCs may be turgid and increase in size (9-10 m)
• In alkaline urine, they may be small or entirely destroyed forming
massive of brownish granules
• In diluted and alkaline urine, the red cell will rupture and release the
hemoglobin, leaving faint colorless cell membrane, and are known as “
ghost” cells (shadow of original cells)
17
18.
18
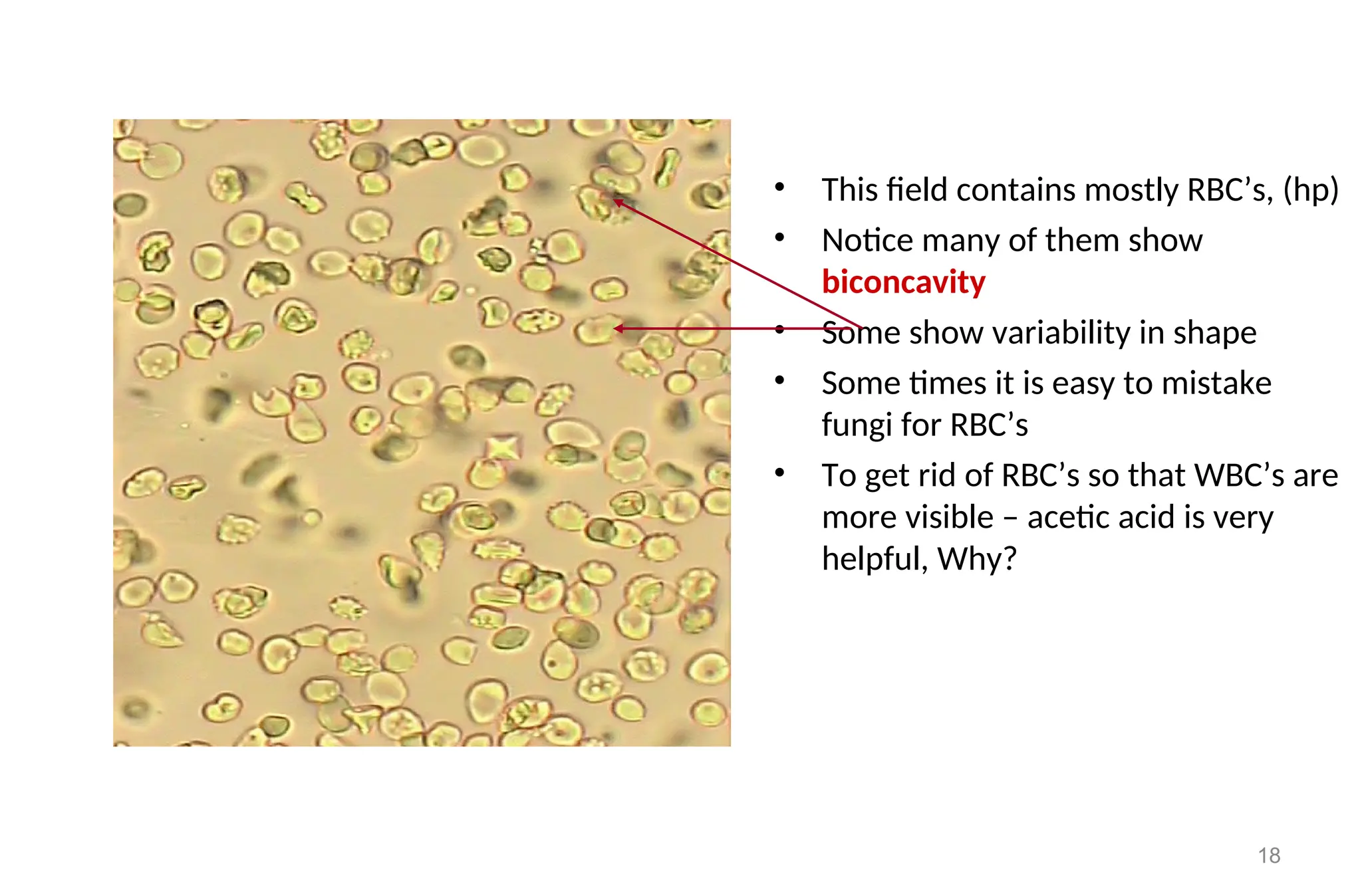
• This fieldcontains mostly RBC’s, (hp)
• Notice many of them show
biconcavity
• Some show variability in shape
• Some times it is easy to mistake
fungi for RBC’s
• To get rid of RBC’s so that WBC’s are
more visible – acetic acid is very
helpful, Why?
19.
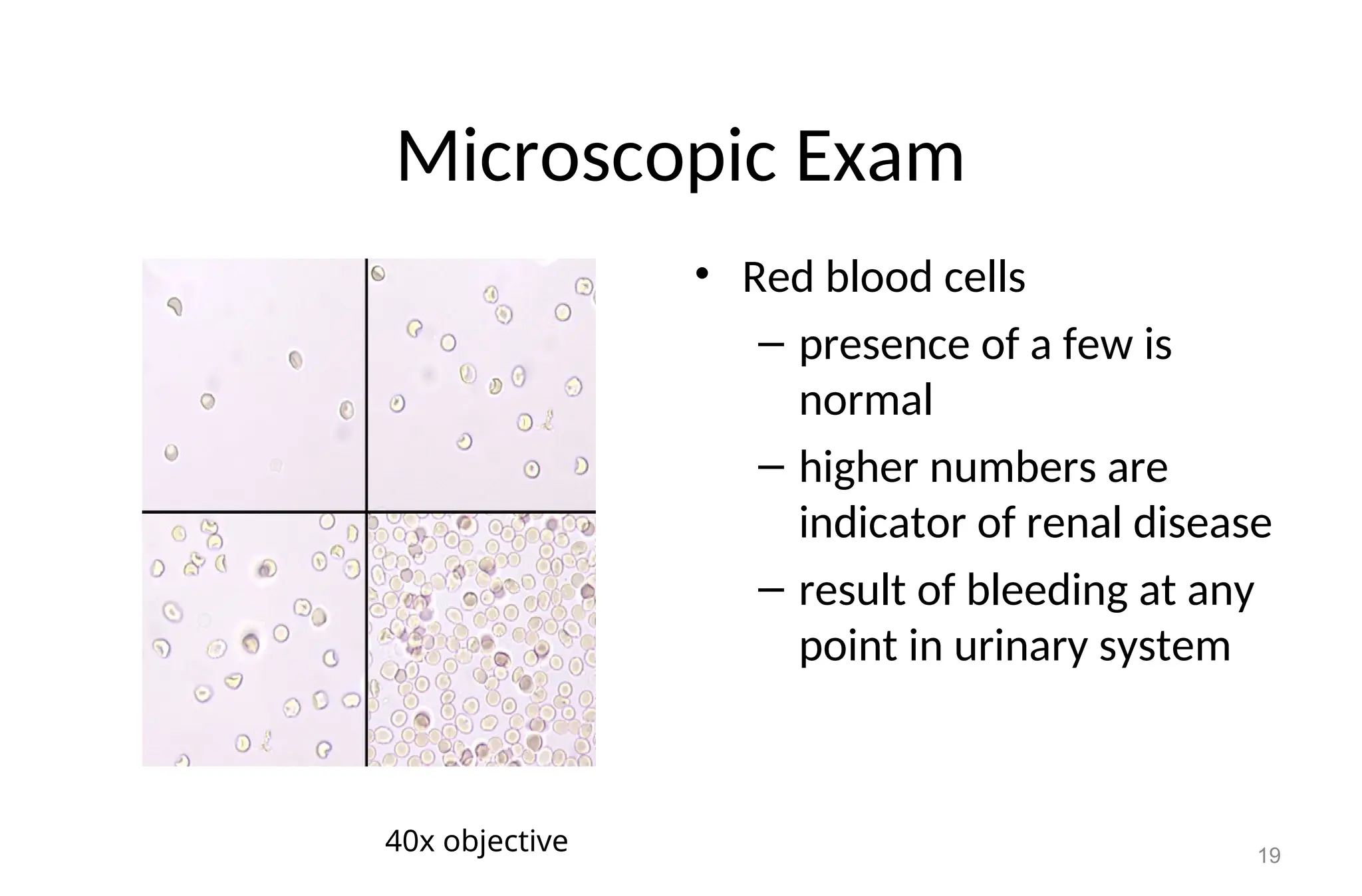
Microscopic Exam
• Redblood cells
– presence of a few is
normal
– higher numbers are
indicator of renal disease
– result of bleeding at any
point in urinary system
19
40x objective
20.
Clinical significance
• Whenthe number of RBCs is found more than their normal range,
usually greater than 5 RBCs/HPF it may indicate:
• Presence of disease conditions in the urinary tract, such as:
– Acute and chronic glomerulonephritis
– Tumor that erode any part of the urinary tract
– Renal stone
– Cystitis
– Prostates
– Trauma of the kidney
– traumatic catheterization
20
21.
Substances confusing withRBCs
• Yeast cells, leukocytes, and bubbles may confuse with red blood
cells
• Differentiate by
• Yeast cells:
– smaller and are oval in shape flattened.
– vary considerably in size with one specimen
– have budding at the surface
• Bubbles (oil droplets)
– vary considerably in size,
– are extremely refractive or shiny
• Leukocytes
– larger and have granular appearance
– upon addition of 2-5% acid the red blood cells will disappear
21
22.
22
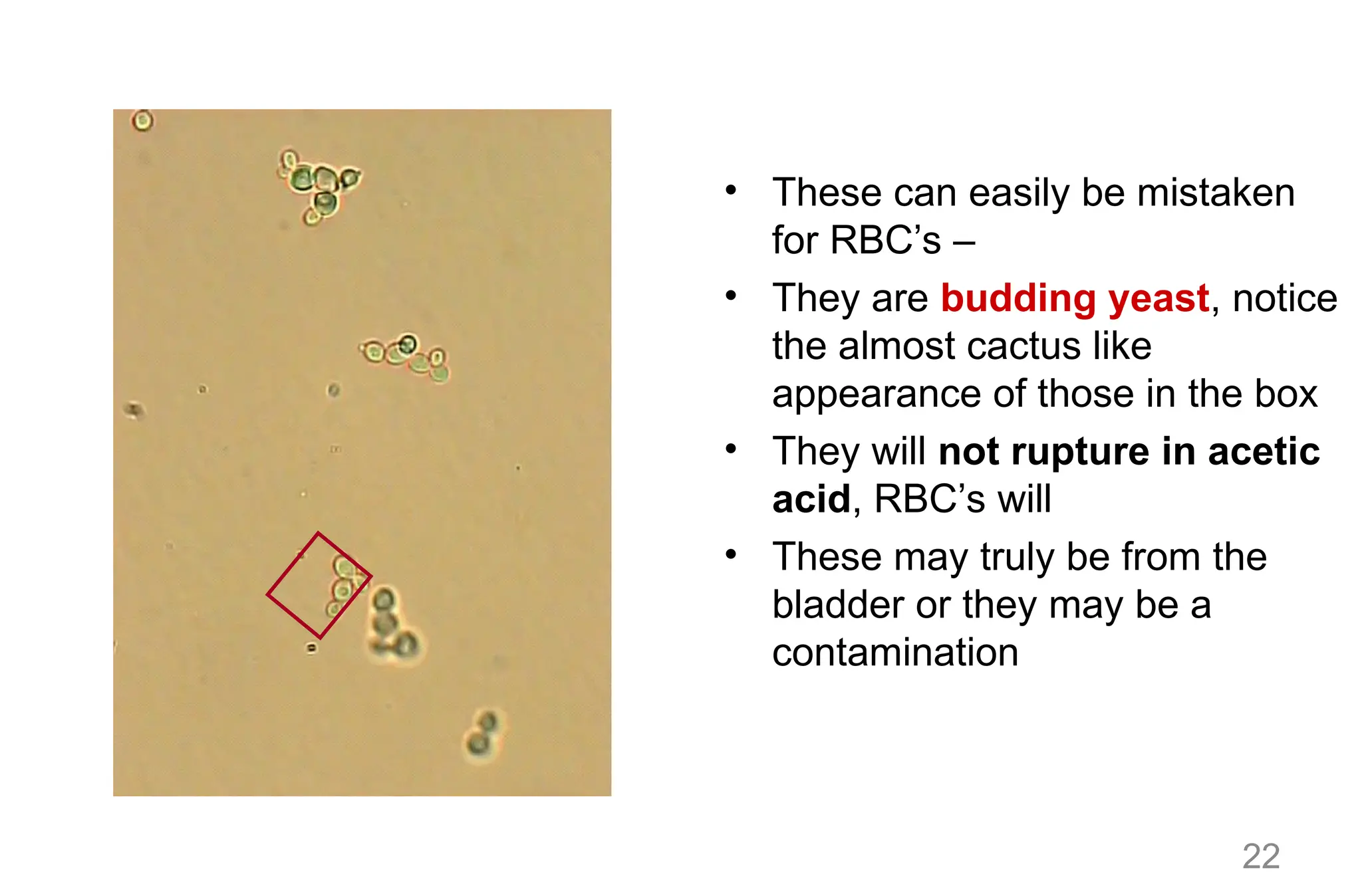
• These caneasily be mistaken
for RBC’s –
• They are budding yeast, notice
the almost cactus like
appearance of those in the box
• They will not rupture in acetic
acid, RBC’s will
• These may truly be from the
bladder or they may be a
contamination
23.
23
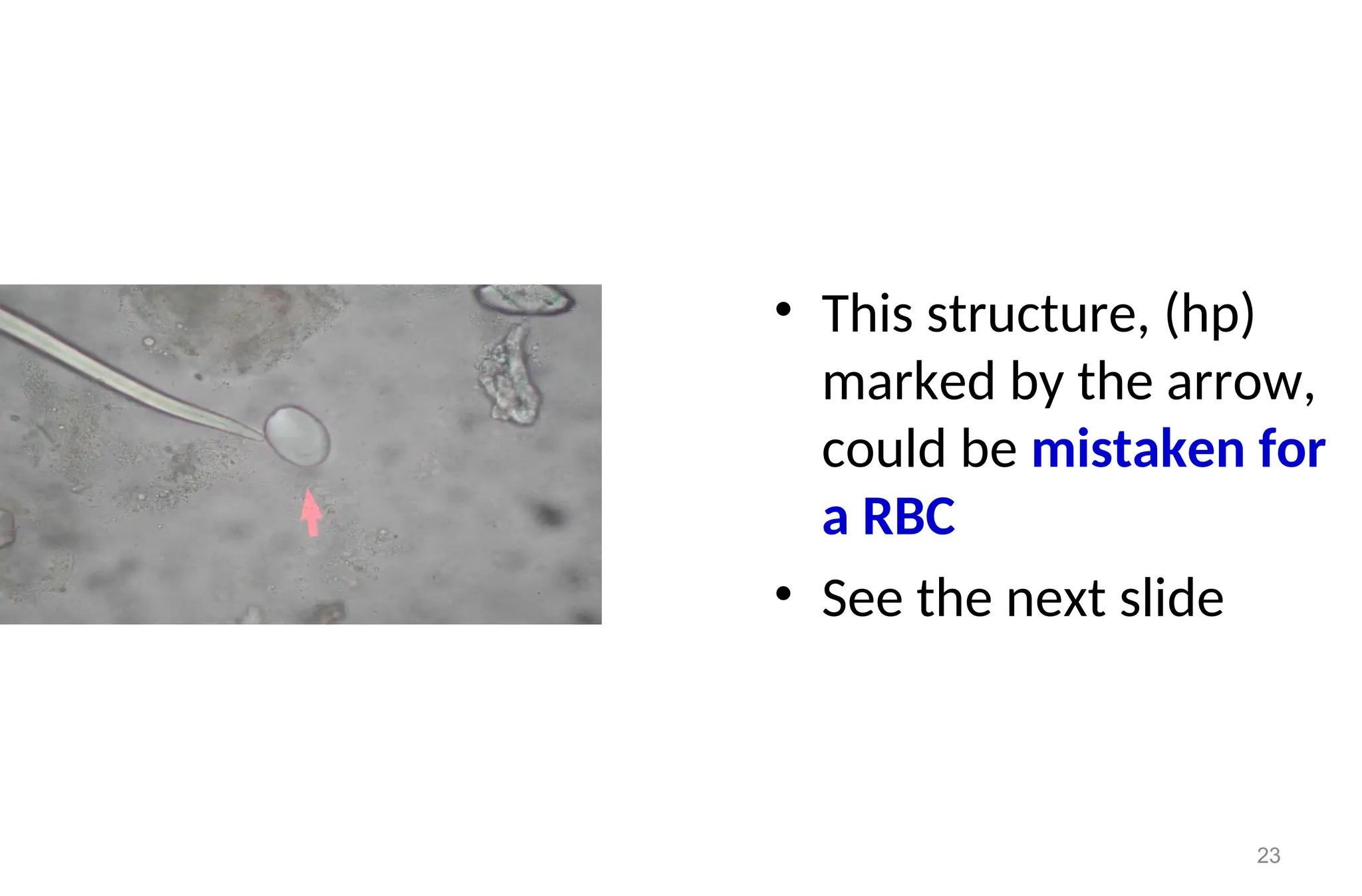
• This structure,(hp)
marked by the arrow,
could be mistaken for
a RBC
• See the next slide
24.
24
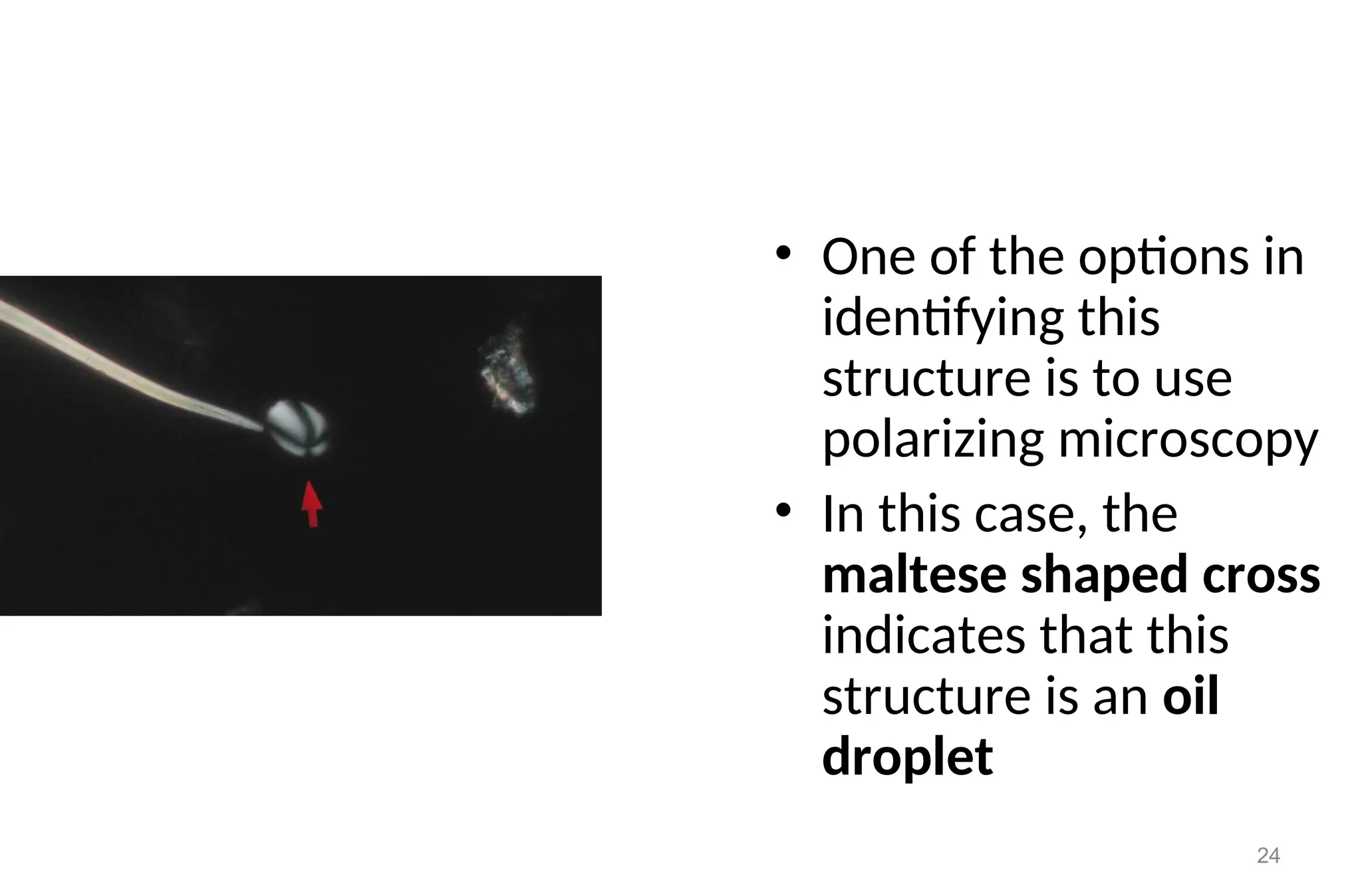
• One ofthe options in
identifying this
structure is to use
polarizing microscopy
• In this case, the
maltese shaped cross
indicates that this
structure is an oil
droplet
25.
Interfering factors:
• Factorsthat may result falsely in high number of RBCs, i.e. without
the presence of actual renal or other normal physiological
disturbances included:
– Menstrual bleeding
– Vaginal bleeding
– Trauma to perianal area in female patients
– Following traumatic catheterization
• Some drugs:
• Aspirin ingestion or over dose
• Anticoagulant therapy over dose
25
26.
LEUKOCYTES (WBCs)
• Normalrange: 0-4 WBC/HPF.
• Appearance: normally, clear granular disc shaped,
• Measure 10-15 m, the nuclei may be visible.
• In alkaline urine, they may increase their size and become irregular.
• Predominantly, polymorph nuclear neutrophils are seen.
• Sometimes because of predominance of neutrophils and the occurrence
of bacterial cell together with polymorphonuclear cells, WBCs are called
pus cells.
• WBCs (pus cells) may be seen in clumps.
26
27.
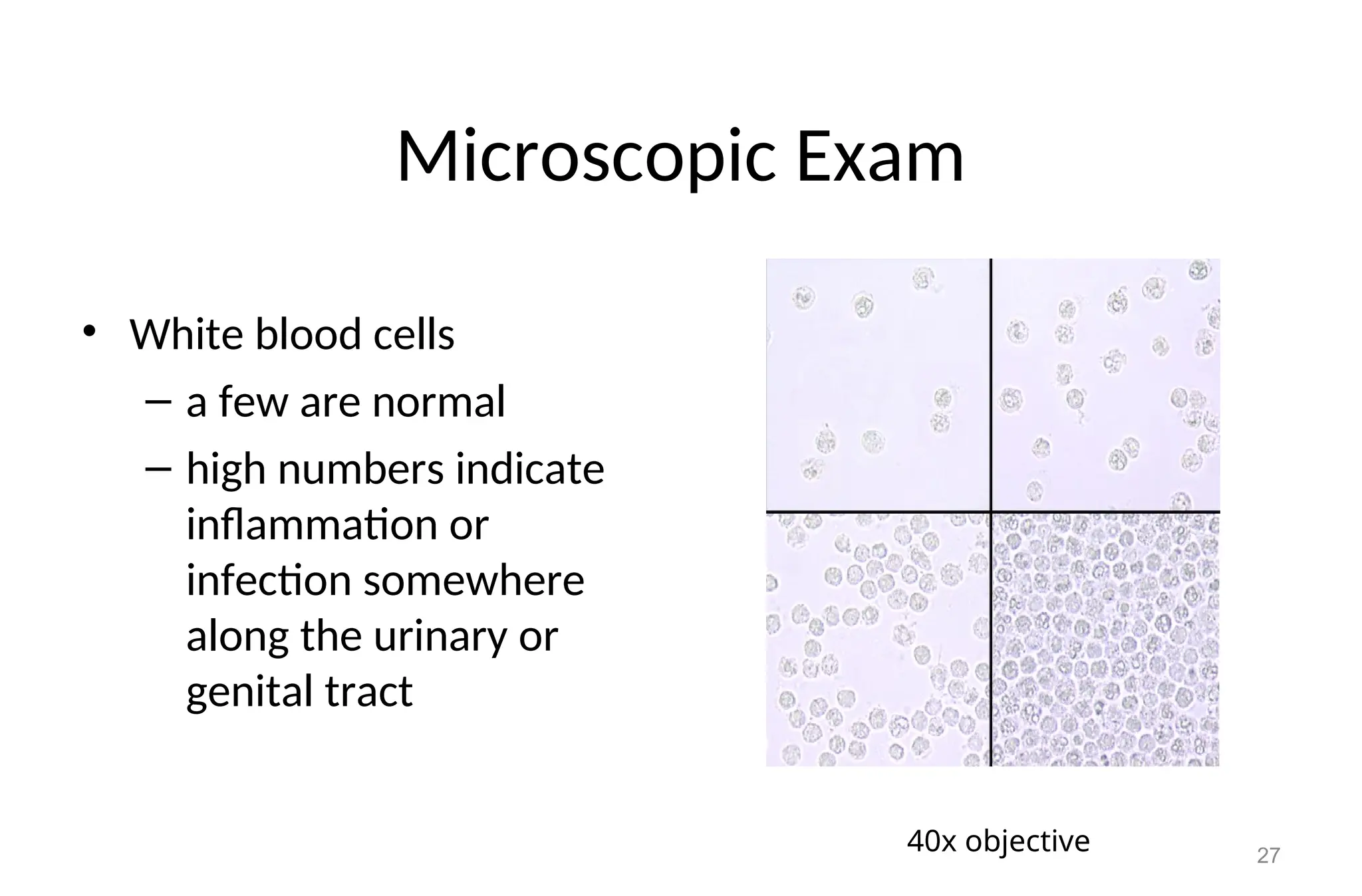
Microscopic Exam
• Whiteblood cells
– a few are normal
– high numbers indicate
inflammation or
infection somewhere
along the urinary or
genital tract
27
40x objective
28.
How to reportthe result of WBCs
• After observing the distribution of leukocytes under 40x objective,
at least 10 fields of microscope
• When 0-5 leukocytes / HPF are seen-- normal
• 5-10 leukocytes / HPF are seen-- few leukocytes / HPF
• 10-20 leukocytes/HPF are seen--->moderate leukocytes/ HPF
• 20-30 leukocytes /HPF are seen ----> many leukocytes / HPF
• Above 30 leukocytes / HPF / are seen - full/field
28
29.
Clinical significance
• Increasednumber of leukocyte urine are seen in case of:
– Urinary tract infection such as renal tuberculosis
– All renal disease
– Bladder tumor
– Cystitis
– Prostates
• Temporarily increased number of leukocytes are also seen during:
– Fever
– After strenuous exercise
29
30.
EPITHELIAL CELLS
Those comingfrom renal cells:
– Size is small as compared to other epithelial cells
– It measures 10 to 18 m in length, i.e., slightly larger than
leukocytes
– Very granular
– Have refractive and clearly visible nucleus
– Usually seen in association with proteins or casts .
30
31.
EPITHELIAL CELLS (cont…)
•Cells from pelvis and urethra of the kidney
Size is larger than renal epithelia’s
Those from pelvis area are granular with sort of tail, while those
from urethra are oval in shape
Most of the time urethral epithelia is seen with together of
leukocytes and filaments (mucus trades and large in number)
Pelvic epithelia’s seen usually with no leukocyte and mucus
trade, and are few in number
31
32.
EPITHELIAL CELLS (cont..)
•Bladder cells
– Are squamous epithelial cells
– Very large in size.
– Shape seems rectangular and often with
irregular border.
– Have single nucleus.
32
33.
33
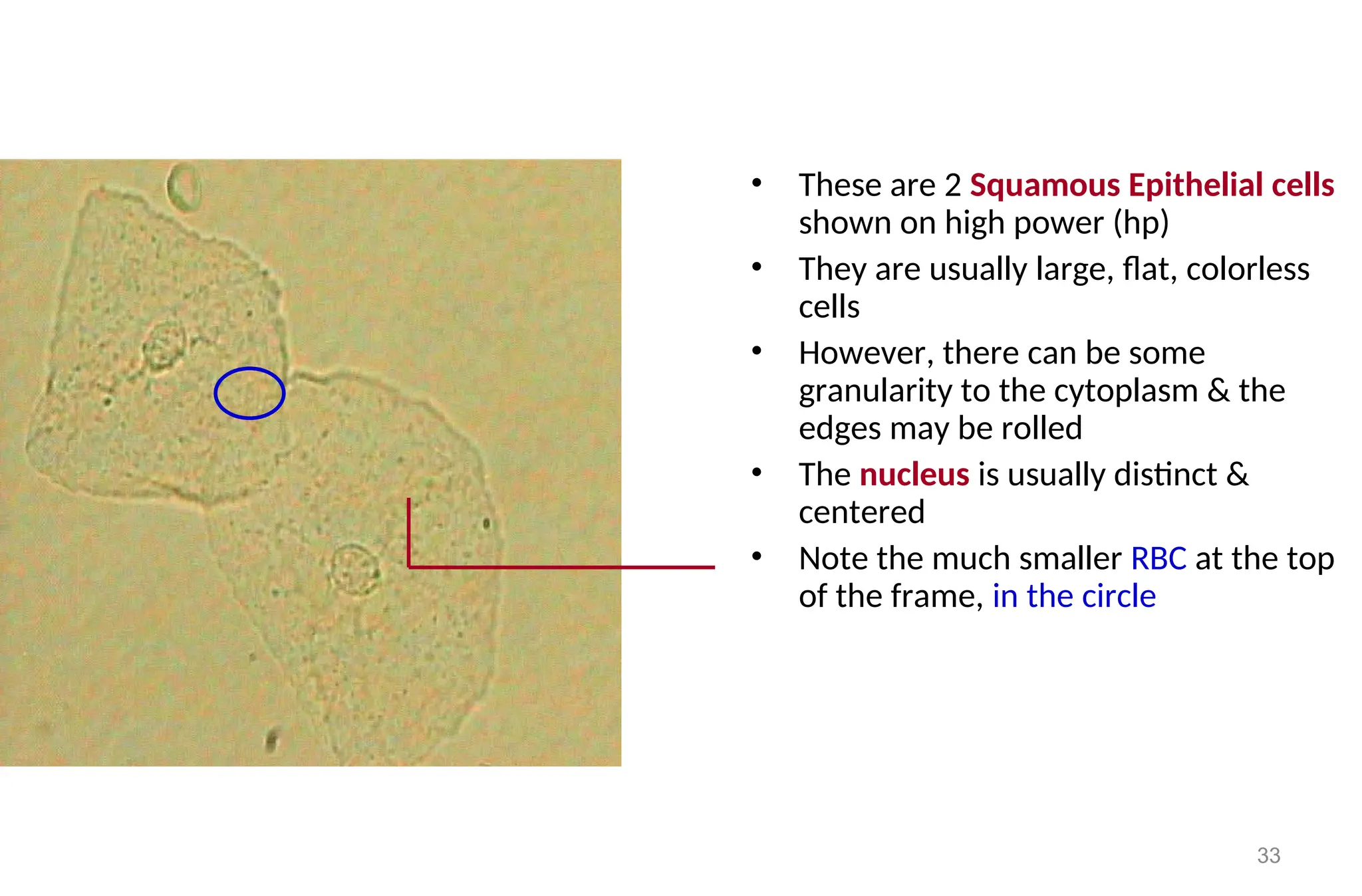
• These are2 Squamous Epithelial cells
shown on high power (hp)
• They are usually large, flat, colorless
cells
• However, there can be some
granularity to the cytoplasm & the
edges may be rolled
• The nucleus is usually distinct &
centered
• Note the much smaller RBC at the top
of the frame, in the circle
34.
Microscopic Exam
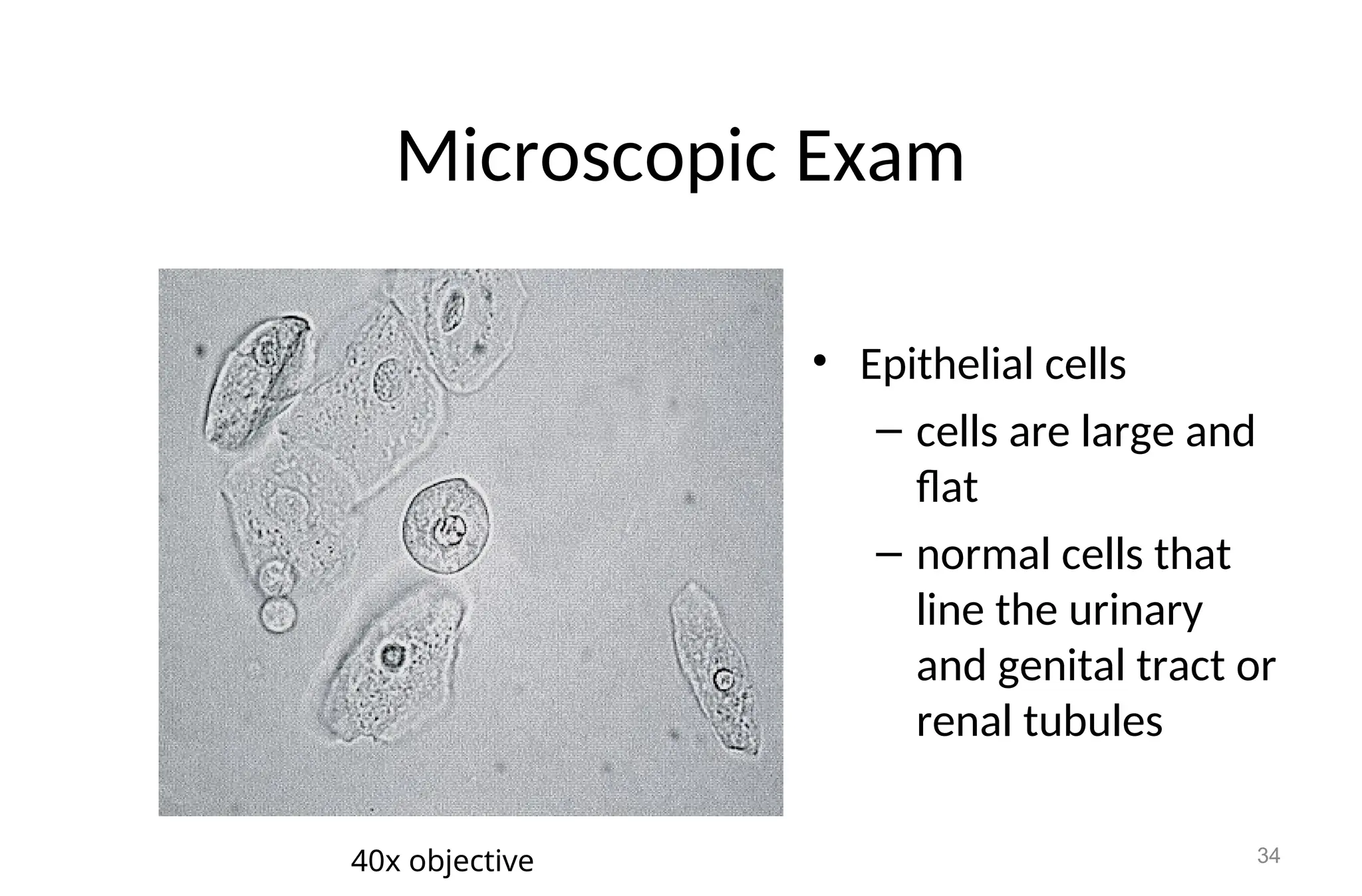
• Epithelialcells
– cells are large and
flat
– normal cells that
line the urinary
and genital tract or
renal tubules
34
40x objective
35.
35
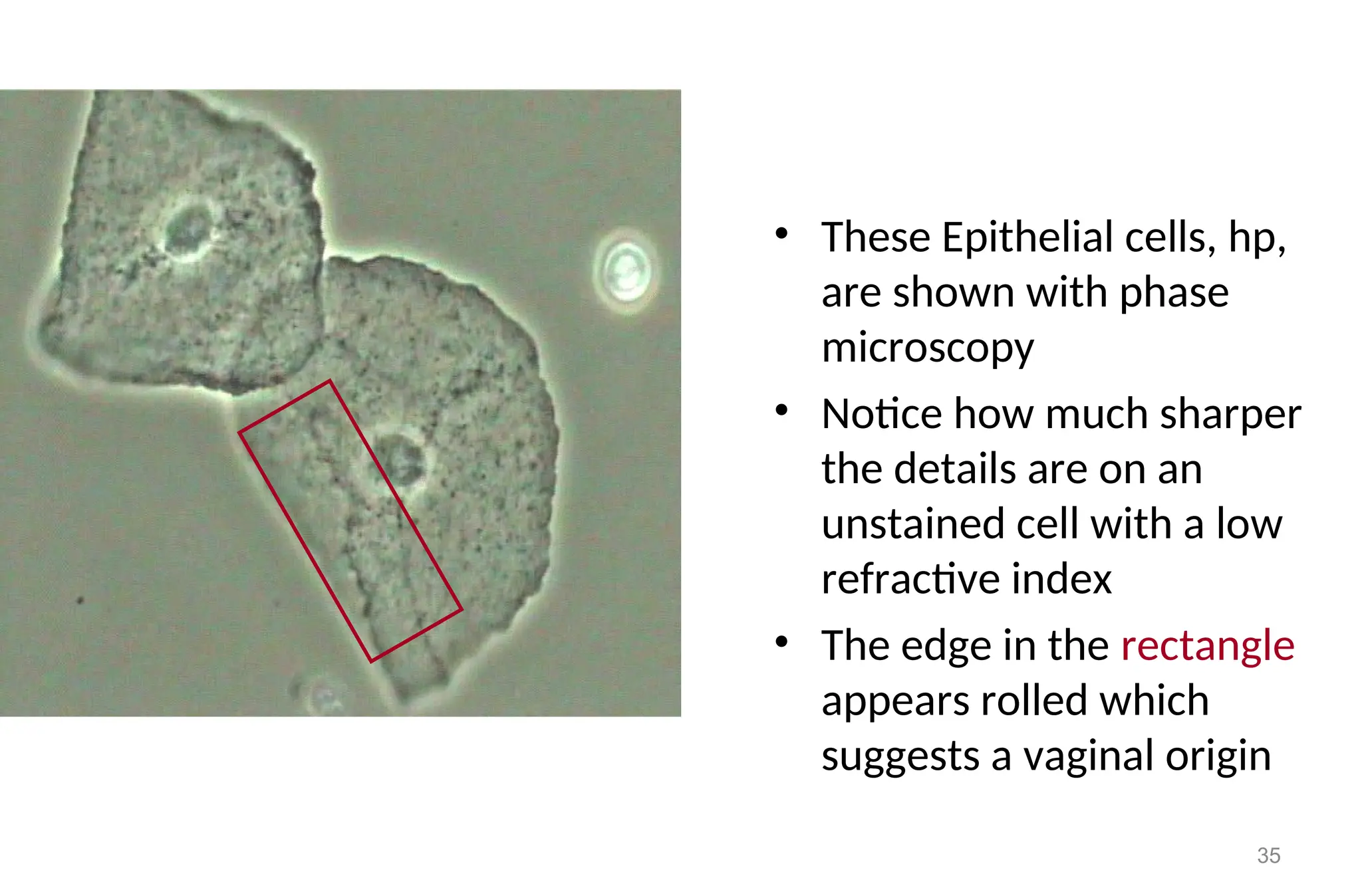
• These Epithelialcells, hp,
are shown with phase
microscopy
• Notice how much sharper
the details are on an
unstained cell with a low
refractive index
• The edge in the rectangle
appears rolled which
suggests a vaginal origin
36.
36
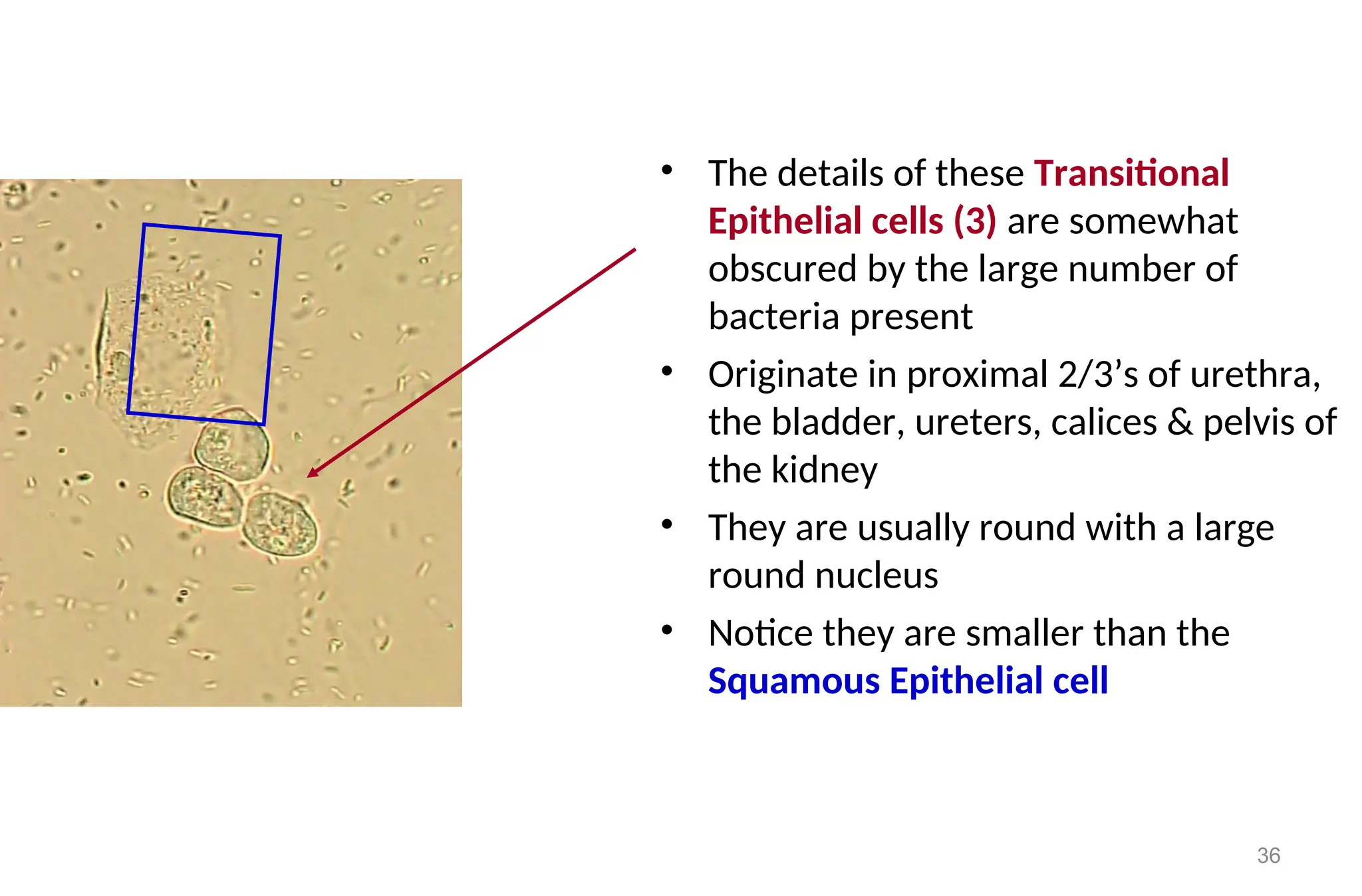
• The detailsof these Transitional
Epithelial cells (3) are somewhat
obscured by the large number of
bacteria present
• Originate in proximal 2/3’s of urethra,
the bladder, ureters, calices & pelvis of
the kidney
• They are usually round with a large
round nucleus
• Notice they are smaller than the
Squamous Epithelial cell
37.
37
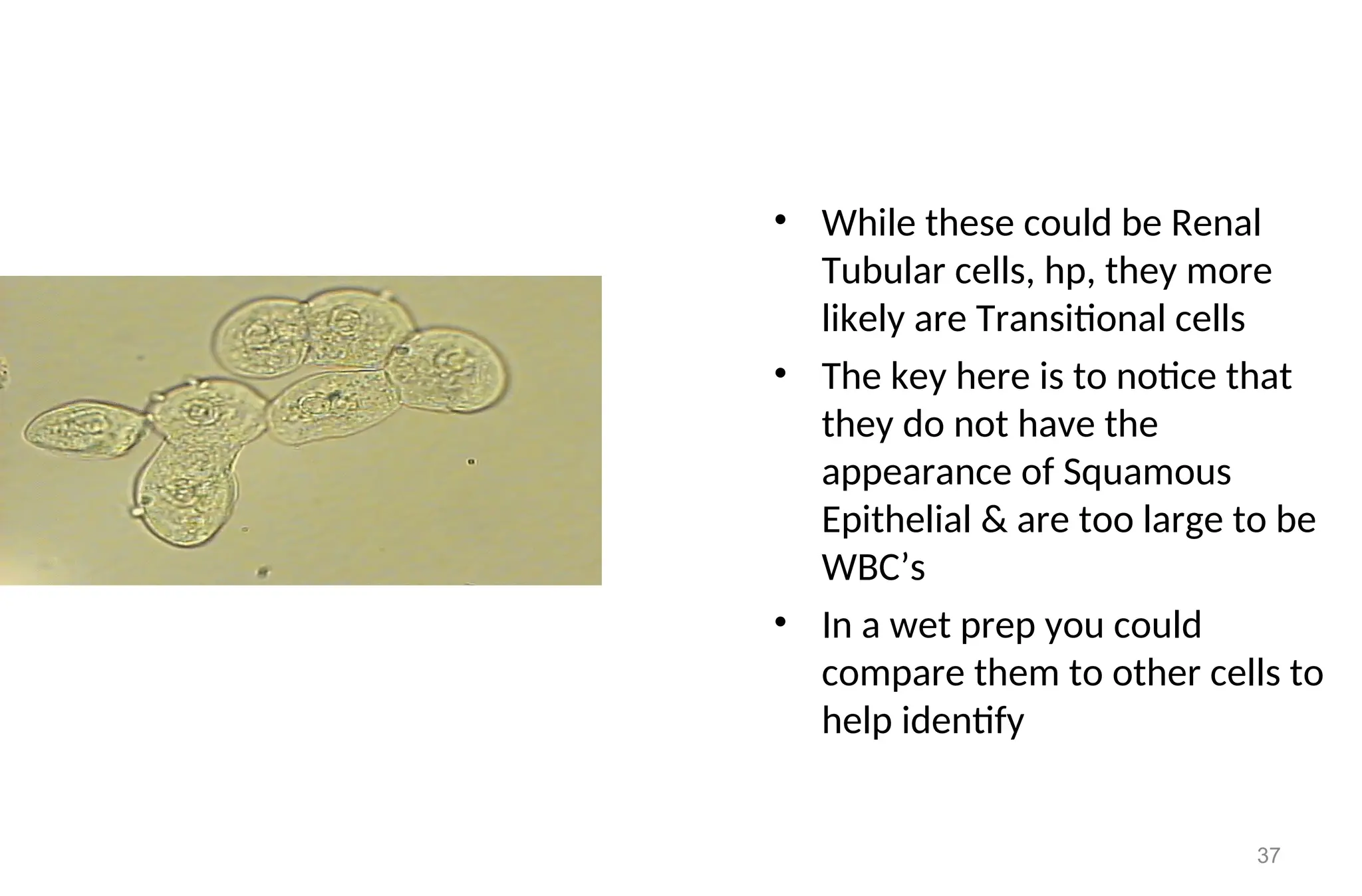
• While thesecould be Renal
Tubular cells, hp, they more
likely are Transitional cells
• The key here is to notice that
they do not have the
appearance of Squamous
Epithelial & are too large to be
WBC’s
• In a wet prep you could
compare them to other cells to
help identify
38.
38
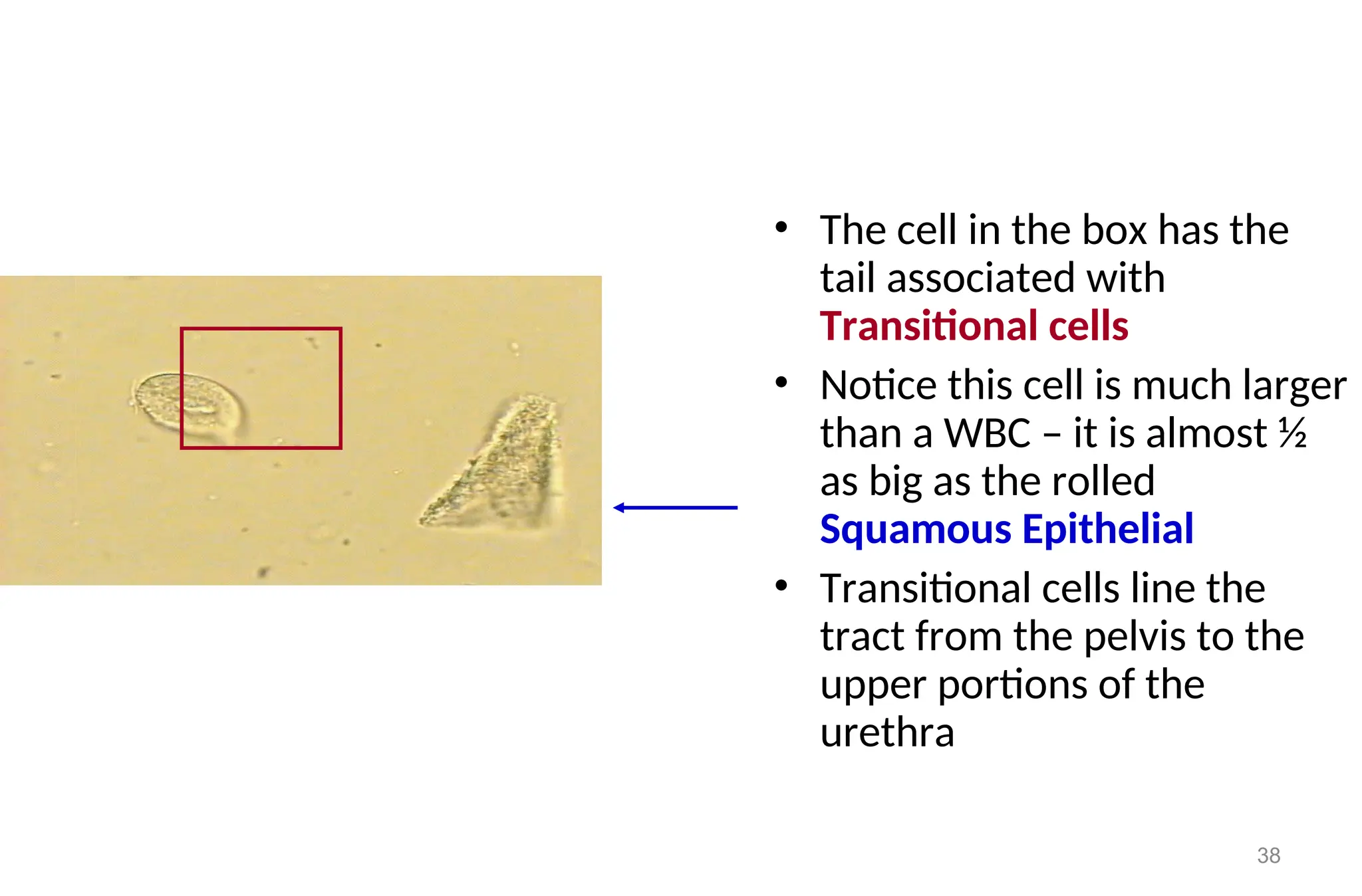
• The cellin the box has the
tail associated with
Transitional cells
• Notice this cell is much larger
than a WBC – it is almost ½
as big as the rolled
Squamous Epithelial
• Transitional cells line the
tract from the pelvis to the
upper portions of the
urethra
39.
Clinical significance
• Presenceof epithelial cells in large number, mostly renal types
may indicate:
– Acute tubular damage
– Acute glomerulonephritis
– Silicate over dose
Note: The presence of large number of epithelial cells with large
number of Leukocytes and mucus trades (filaments) may indicate
Urinary Tract Infections (UTI).
39
40.
Reporting of epithelialcells
• Epithelial cells distribution reported after looking under 10x
objective of the microscope.
• Usually they are reported semi quantitatively by saying
– 1-3 epithelial cells /LPF
– 2-4 epithelial / LPF
– 6-14 epithelial / LPF
– 15-25 epithelial/ LPF
– Full of epithelial cells / LPF when the whole field of 10 x
objective covered by epithelial cells.
40
41.
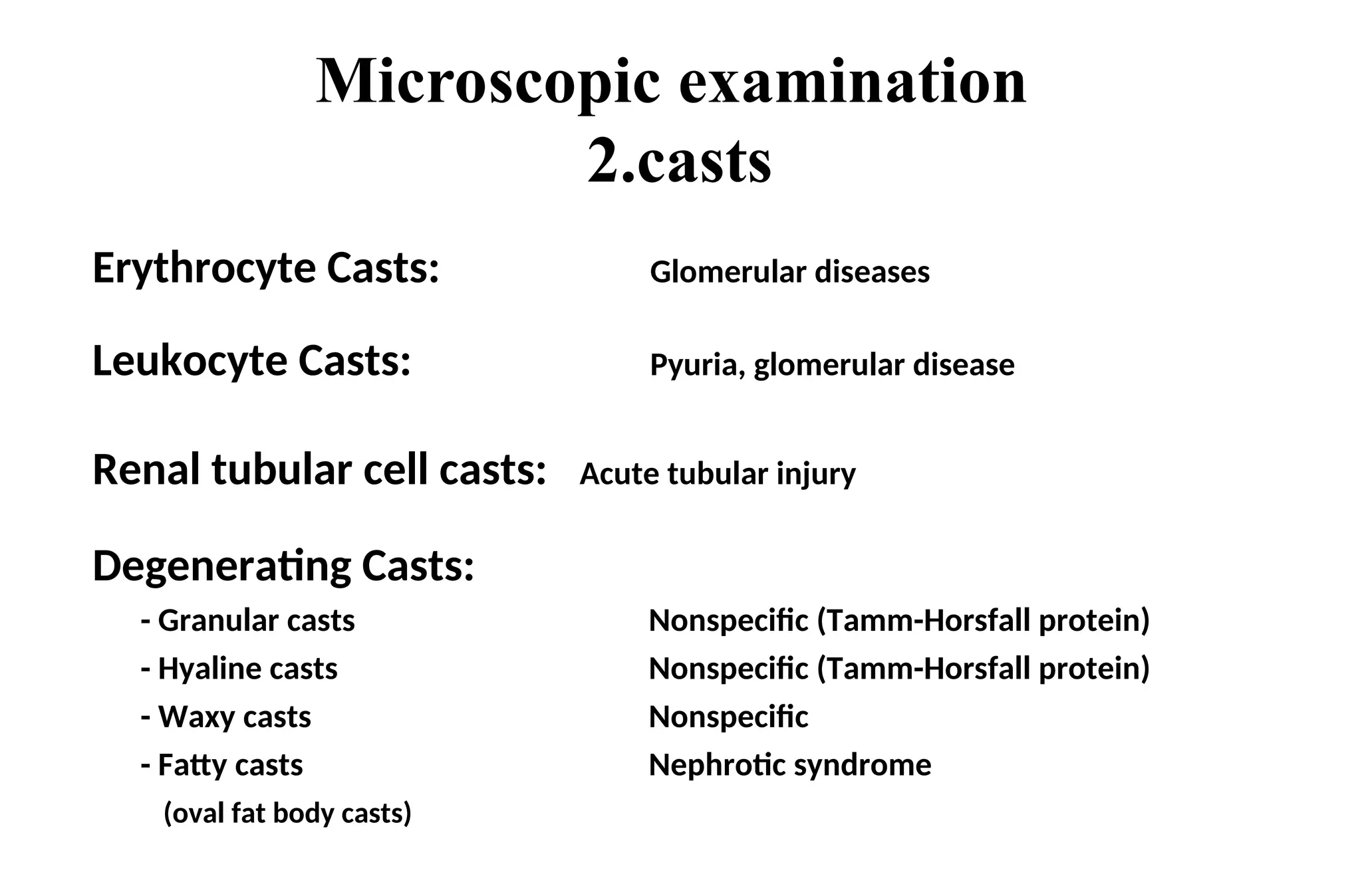
Casts
Introduction:
Castsare long cylindrical structures that result from the solidification
of material within the lumen of the kidney tubules.
Formed by precipitation of proteins, and aggregation of cells within
the renal tubules.
Most of them dissociate in alkaline urine, and diluted urine (specific
gravity 1.010) even in the presence of Proteinuria.
Most of them are transparent.
• Pathological Conditions that favors for the creation of casts include
– The presence of protein constituents in the tubular urine
– Increase acidification
– increase osmolar concentration
41
42.
• Definition :Microscopic, cylindrically shaped formed
elements of the urinary sediment (protein, cells,
debris) that have been molded in the distal tubule or
the collecting duct.
• Formation factors:
– proteinuria : Albumin, mucoprotein (THP)
– high salt concentration, and low pH
– low flow rate, enough alternate nephron
casts
43.
Casts cont’d…
Mosturinary casts are formed either in the distal
convoluted tubules or in the collecting ducts, because urine more
concentrated and maximally acidified here.
But rare conditions such as ,in myeloma, casts may be found in the
proximal convoluted tubules.
Casts formed in the collecting tubules tends to be very
broad, and usually indicates the significant reduction in
the functional capacity of the nephron and indicate
severe renal damage.
43
44.
CASTS (cont…)
• Majorcasts types:
– hyaline
– epithelial
– white blood cell, and. red blood cell casts
– granular (coarse and fine). waxes, Fatty
44
Casts in UrinarySediment
• Casts in urinary sediment is an important aid in the differential
diagnosis of renal disease
• Pure Hyaline casts may be seen in Proteinuria from a variety of
causes.
• Small Hyaline cast seen transiently may occur with marked exercise
or febrile conditions
• Casts with inclusions, such as RBC’s or WBC’s may be formed
without a protein matrix
46
47.
Casts in UrinarySediment
• Correctly identifying casts in urinary sediment is an important
aid in the differential diagnosis of renal disease
• Pure Hyaline casts may be seen in proteinuria from a variety
of causes. Small #’s, seen transiently may occur with marked
exercise or febrile conditions
• Casts with inclusions, such as RBC’s or WBC’s may be formed
without a protein matrix
48.
Hyaline Casts
• Allhyaline cast have a precipitated protein matrix, so there
has to be renal Proteinuria for these to be formed
• The Proteinuria is predominately Tamm-Horsfall
mucoprotein, the later being secreted by cells lining the distal
parts of the nephron
• Low pH & increased electrolyte concentration readily
precipitate Tamm-Horsfall protein
48
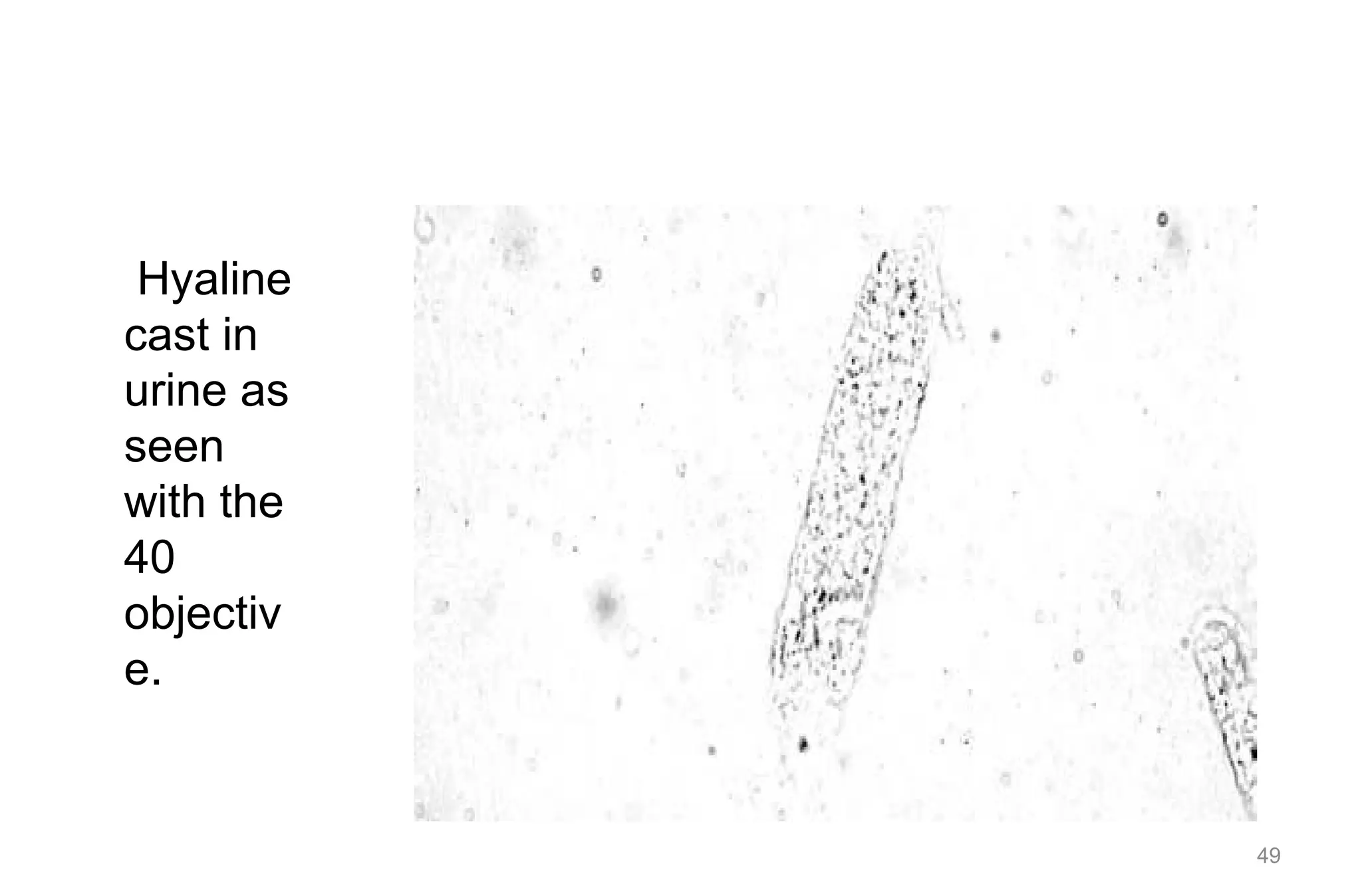
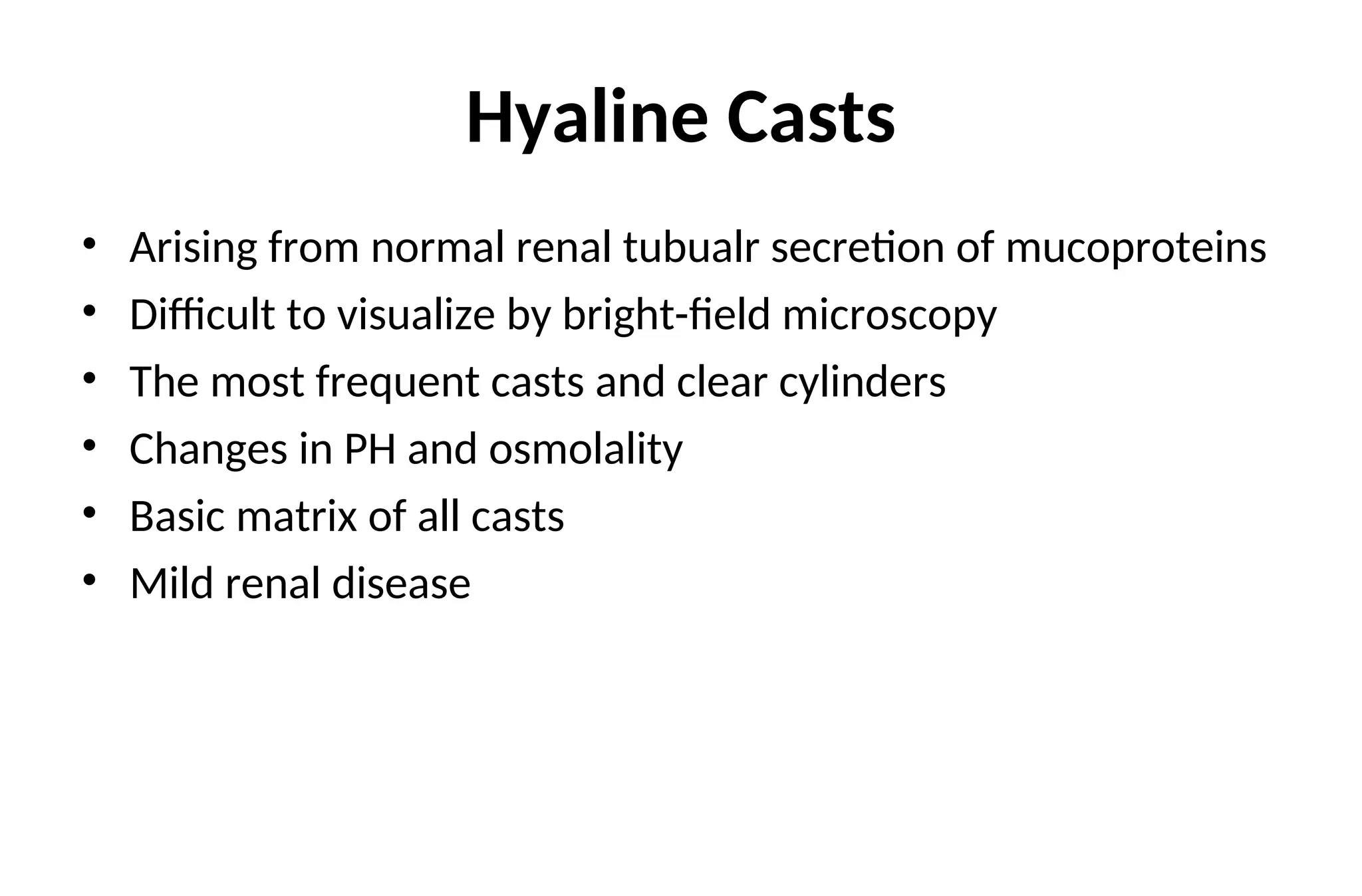
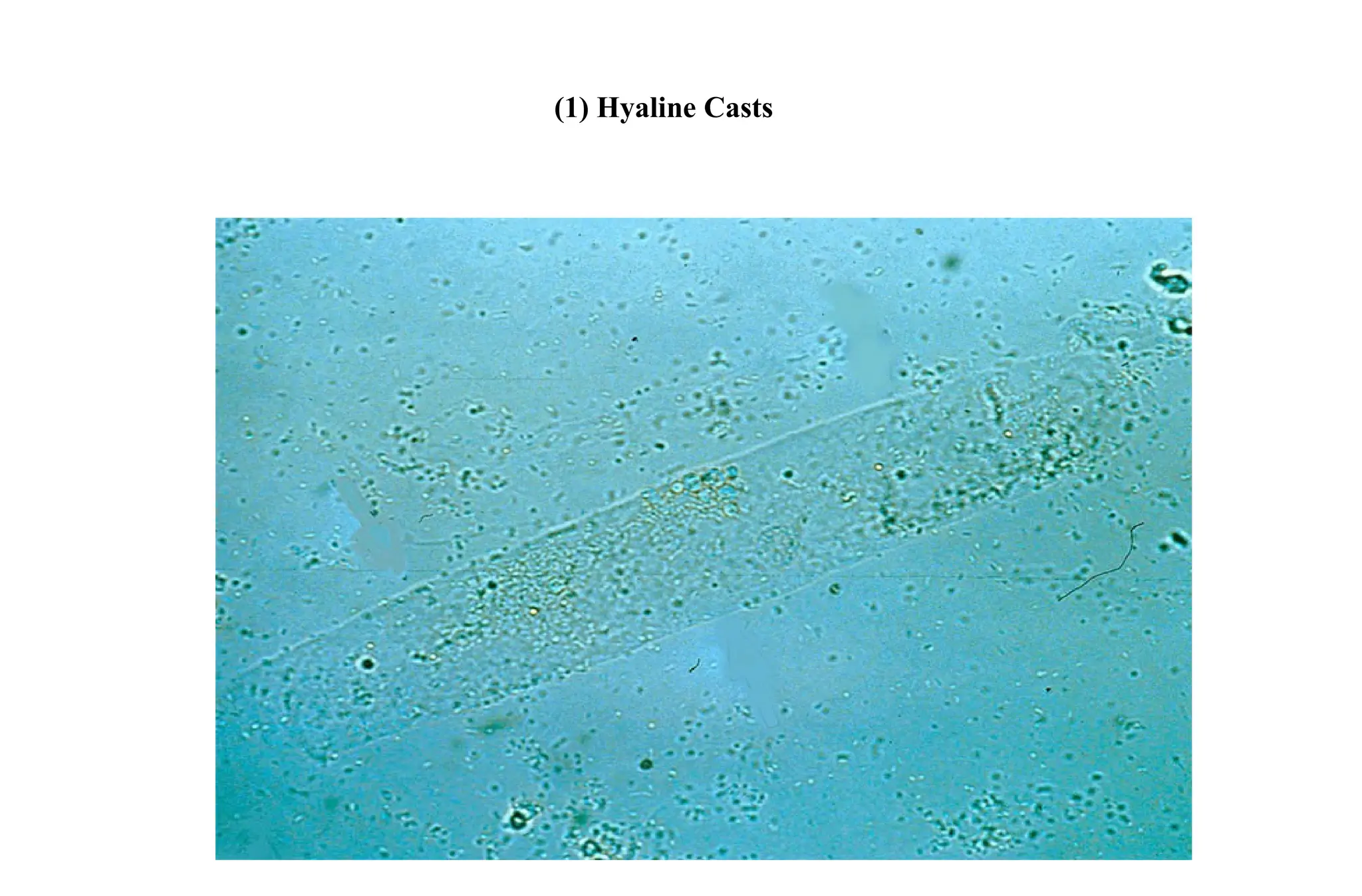
Hyaline Casts
• Arisingfrom normal renal tubualr secretion of mucoproteins
• Difficult to visualize by bright-field microscopy
• The most frequent casts and clear cylinders
• Changes in PH and osmolality
• Basic matrix of all casts
• Mild renal disease
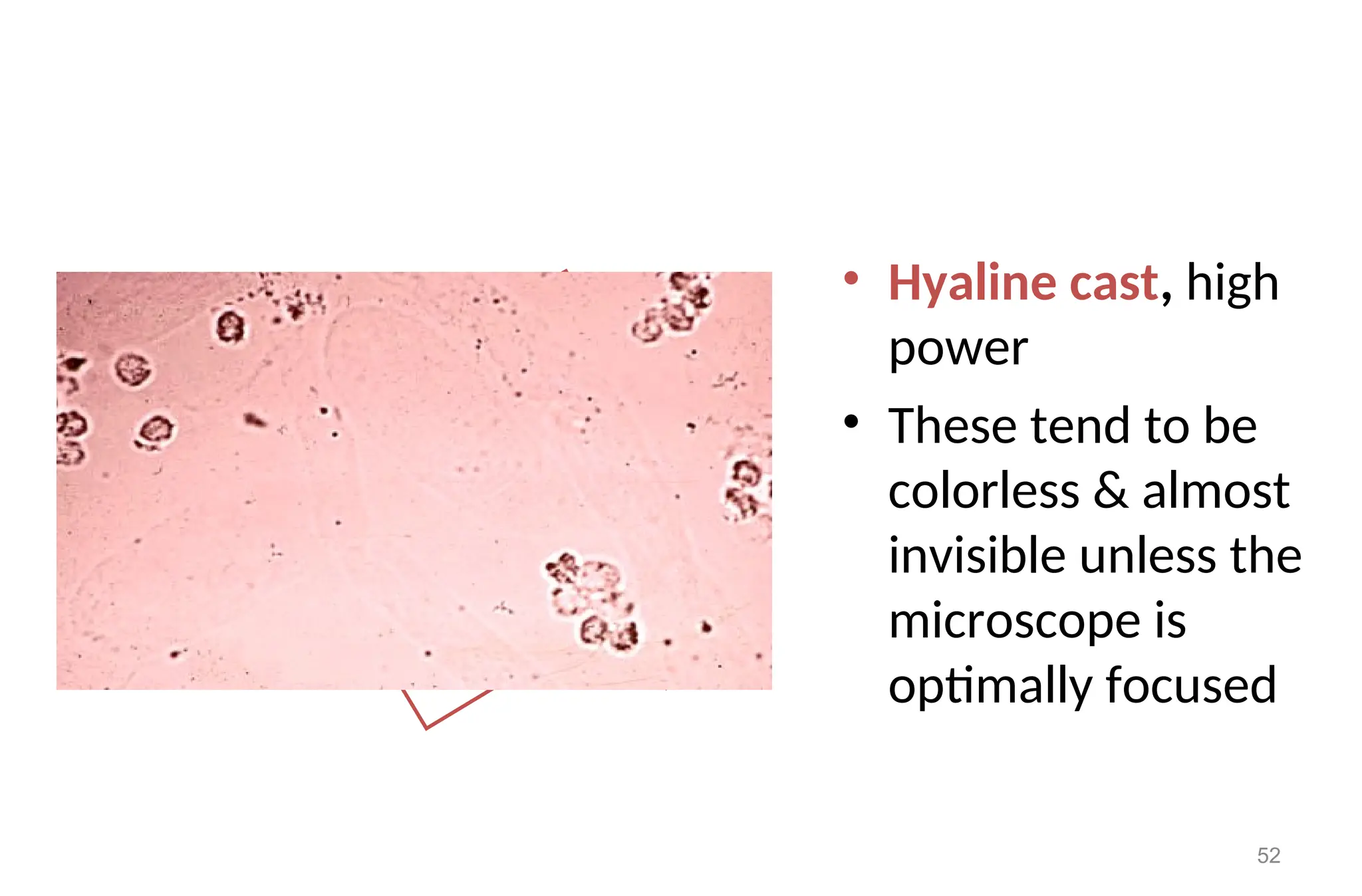
• Hyaline cast,high
power
• These tend to be
colorless & almost
invisible unless the
microscope is
optimally focused
52
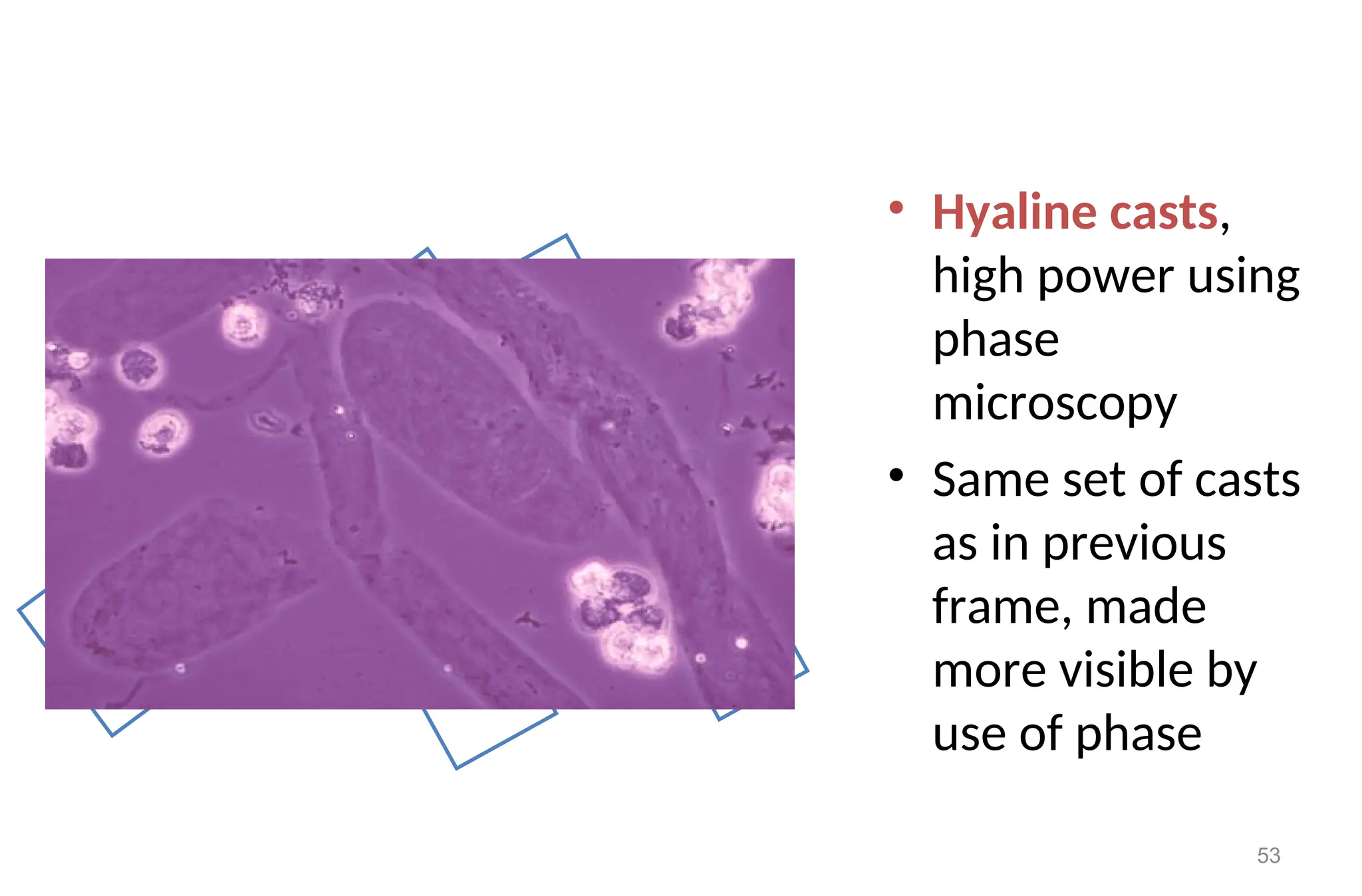
53.
• Hyaline casts,
highpower using
phase
microscopy
• Same set of casts
as in previous
frame, made
more visible by
use of phase
53
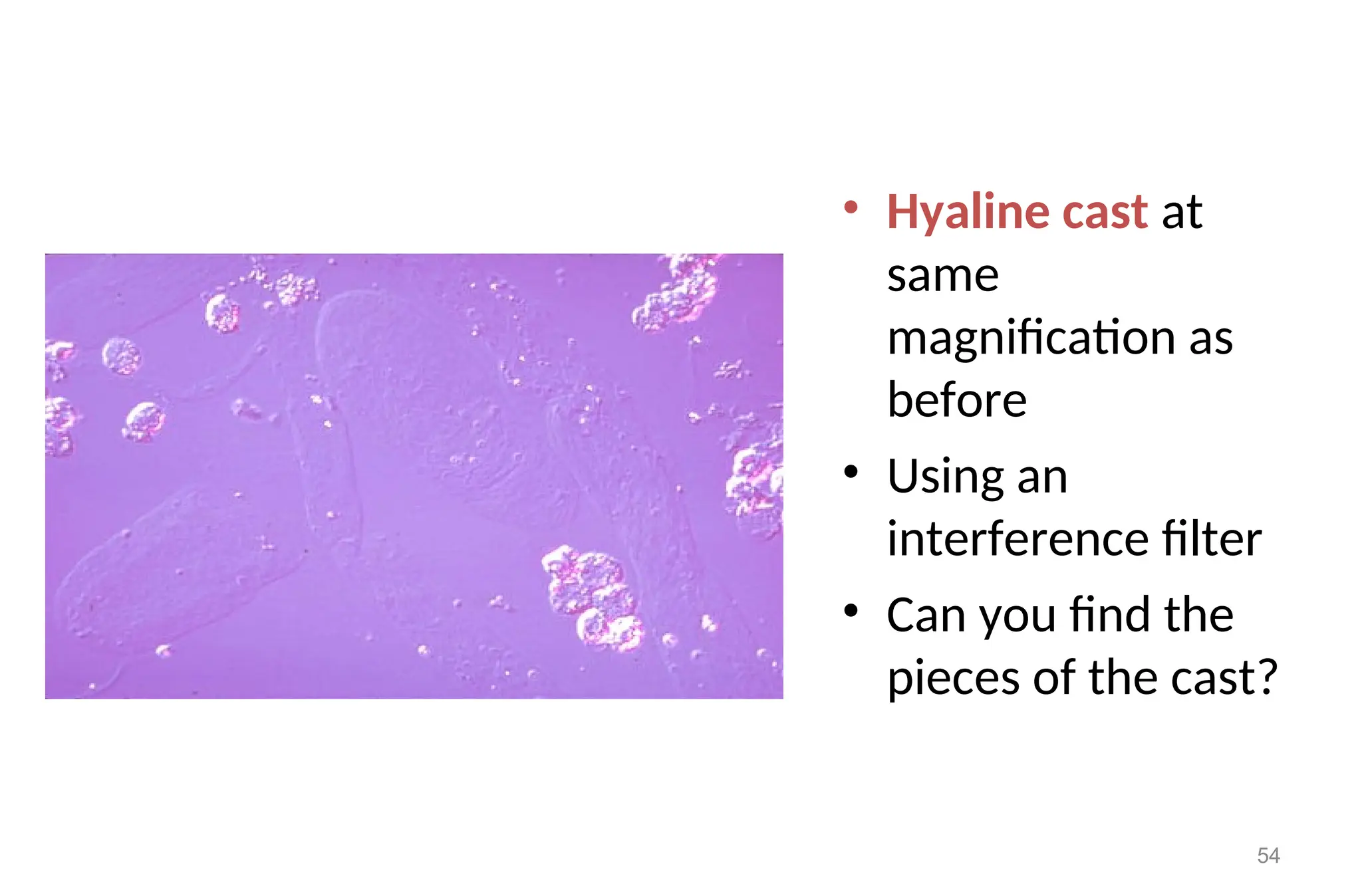
54.
• Hyaline castat
same
magnification as
before
• Using an
interference filter
• Can you find the
pieces of the cast?
54
55.
Clinical Implication
• Presenceof large number of hyaline casts may show possible
damage of glomerular capillary membrane. This damage permits
leakage of protein through glomerulus and result in precipitate
and gel formation (i.e. hyaline casts) in the tubule. Thus this may
indicate:
• Nephritis
• Meningitis
• Chronic renal disease
• Congenital heart failure
• Diabetic nephropathy
55
56.
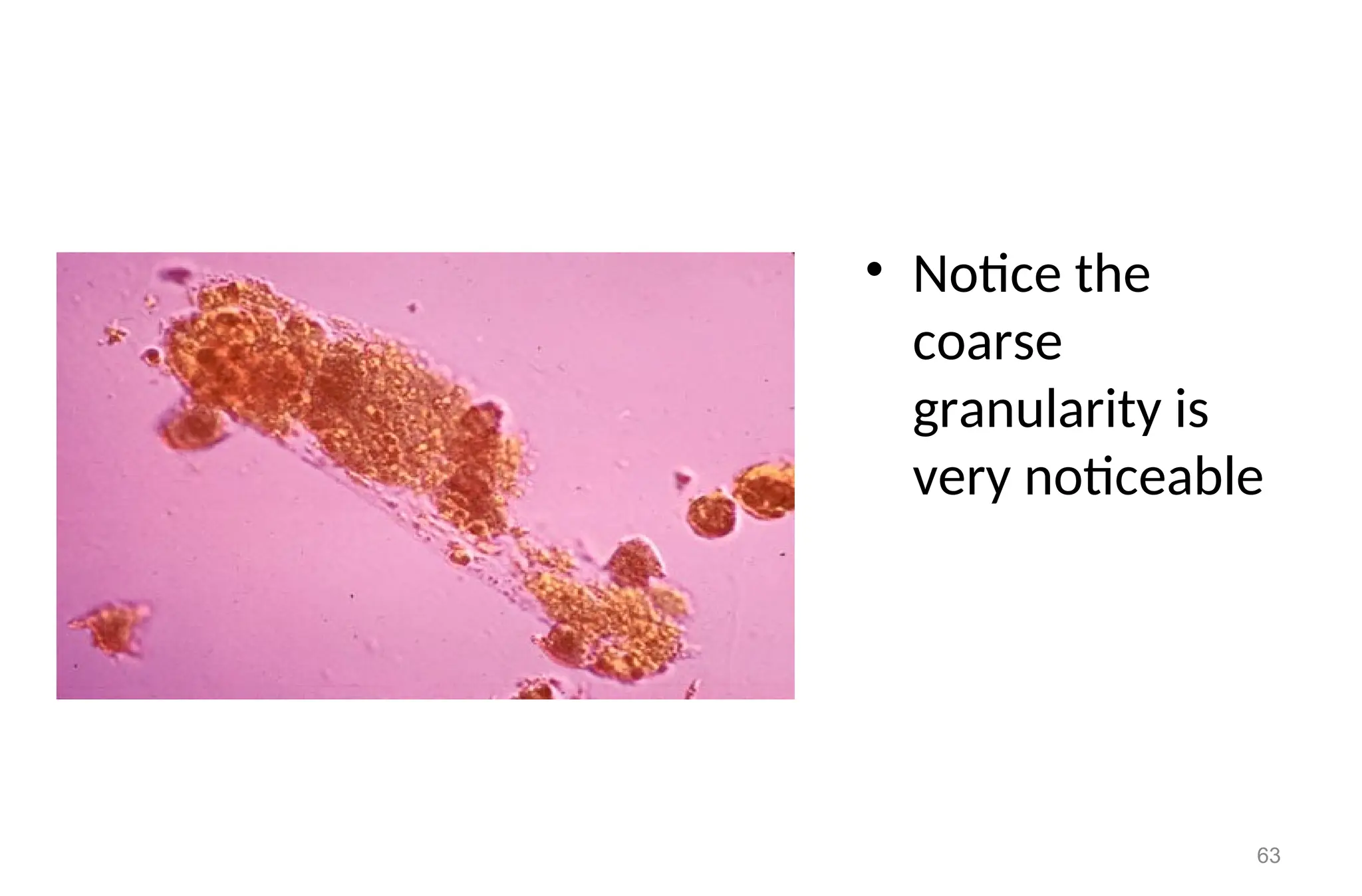
Granular cast
Moresimilar in appearance with hyaline casts and in which
homogenous, course granules are seen.
More dense (opaque) than hyaline cast.
Shorter and broader than hyaline casts.
May represent the first stage of epithelial cell cast degeneration.
Based on the amount and type of granules, divided into:
fine (which may appear grey or pale yellow in color)
course granular casts ( which may appear as darker).
56
57.
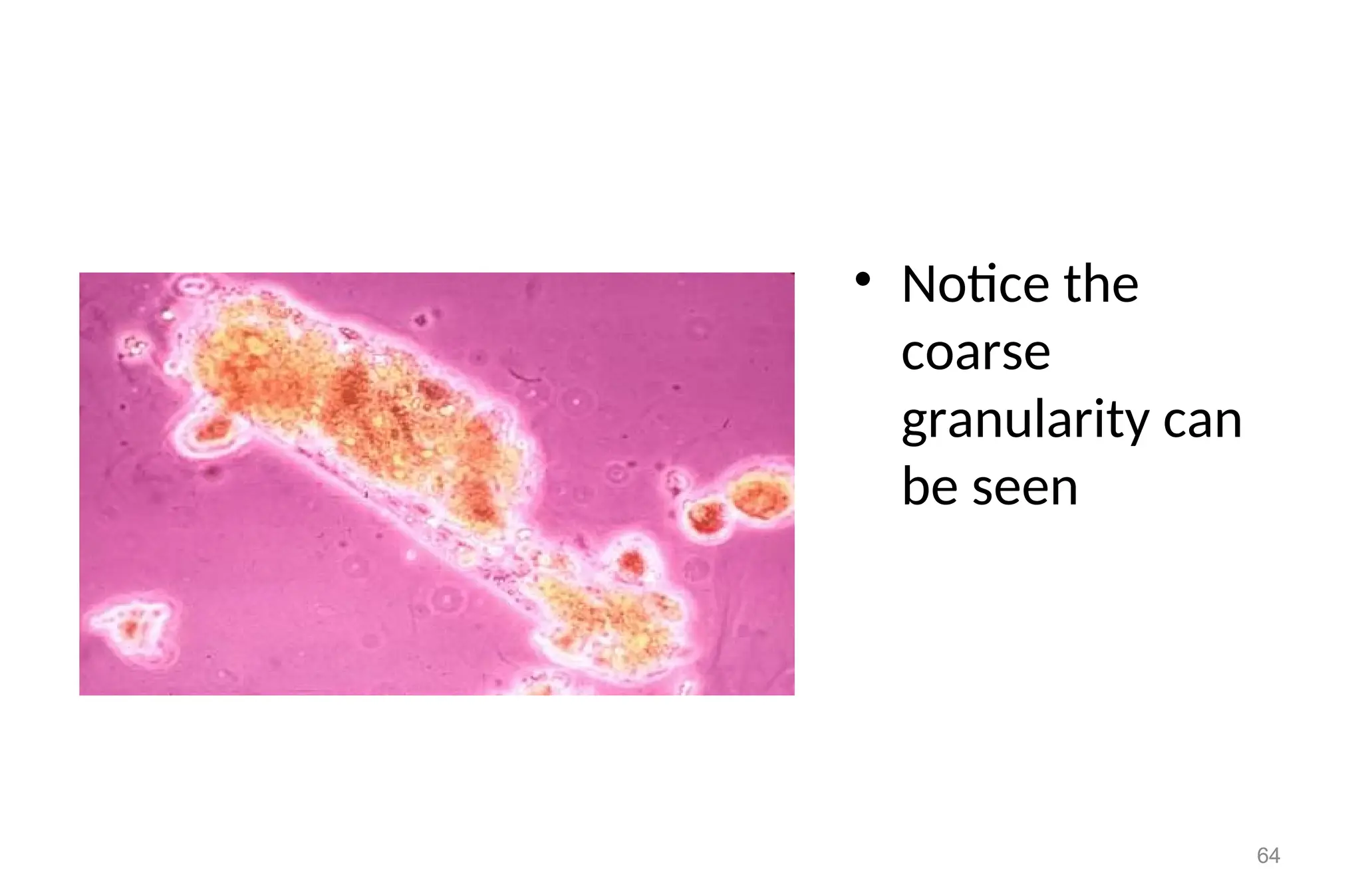
Granular Casts
• Ifcellular casts stay within the tubules of the nephron due to
prolonged stasis, the cells will begin to degenerate
• These casts are referred to as Finely Granular or Coarsely
Granular Casts
• Usually the original type of cell entrapped cannot be
determined unless the cells were RBC & hgb remains
57
58.
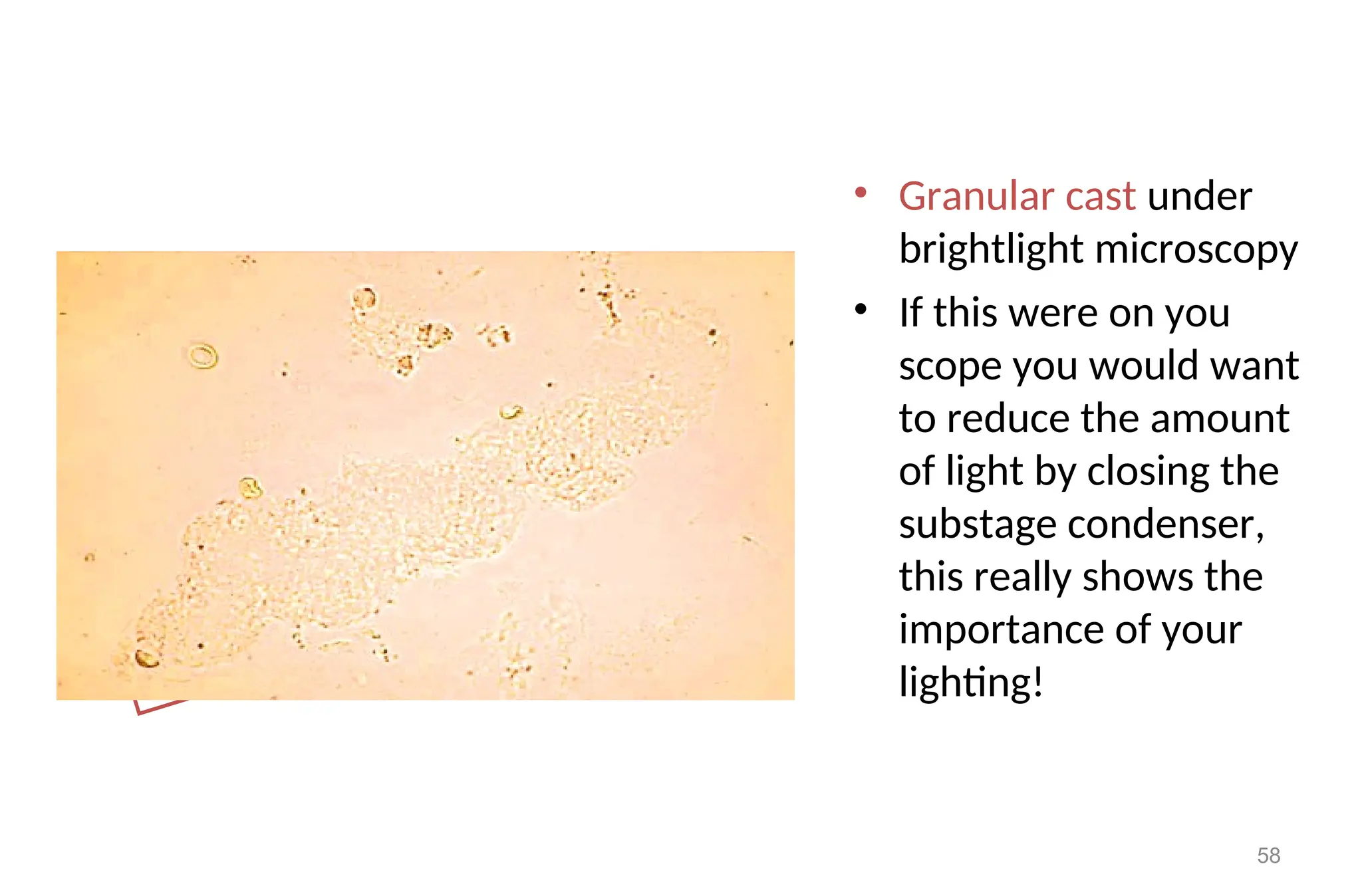
• Granular castunder
brightlight microscopy
• If this were on you
scope you would want
to reduce the amount
of light by closing the
substage condenser,
this really shows the
importance of your
lighting!
58
59.
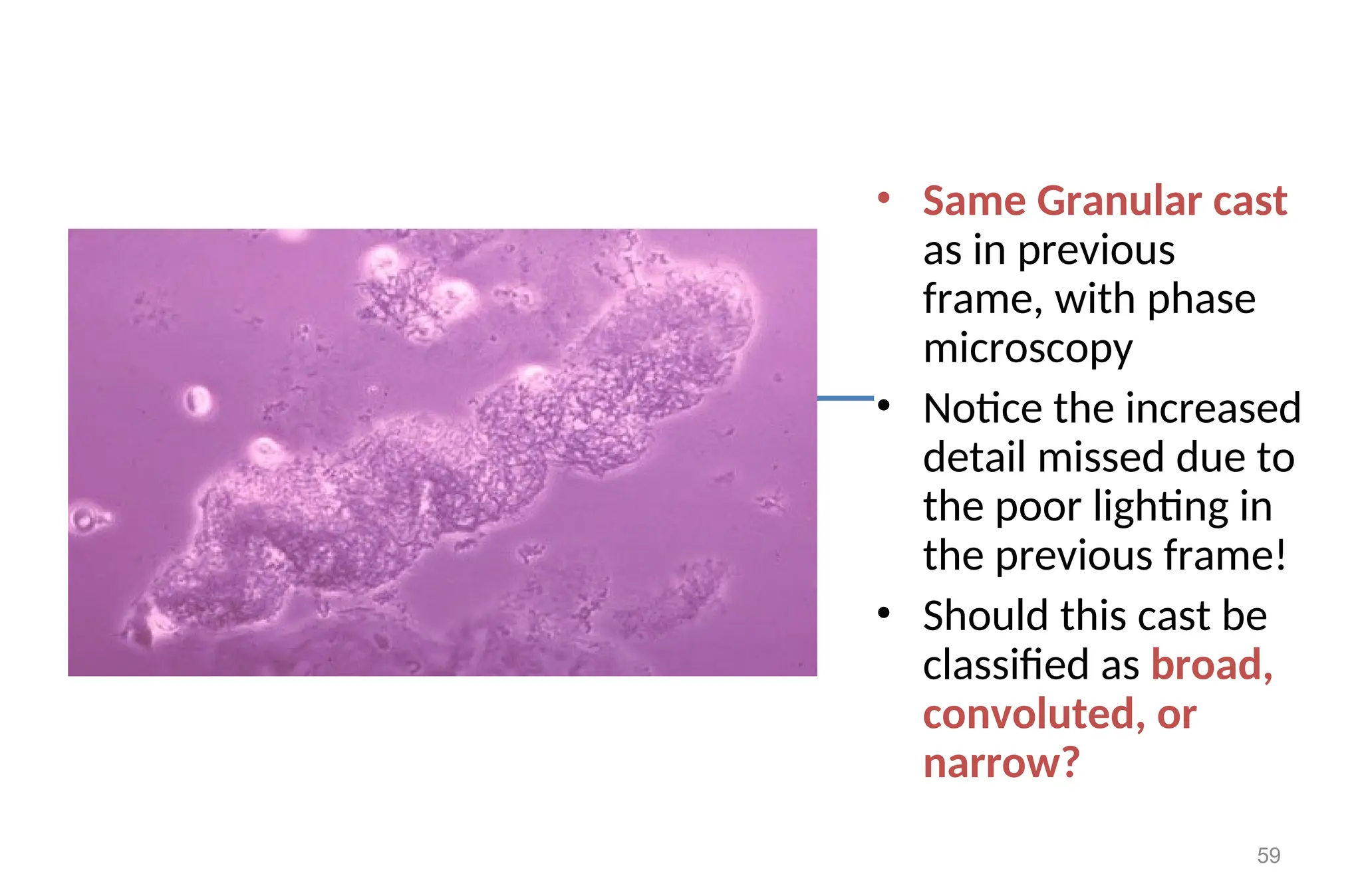
• Same Granularcast
as in previous
frame, with phase
microscopy
• Notice the increased
detail missed due to
the poor lighting in
the previous frame!
• Should this cast be
classified as broad,
convoluted, or
narrow?
59
60.
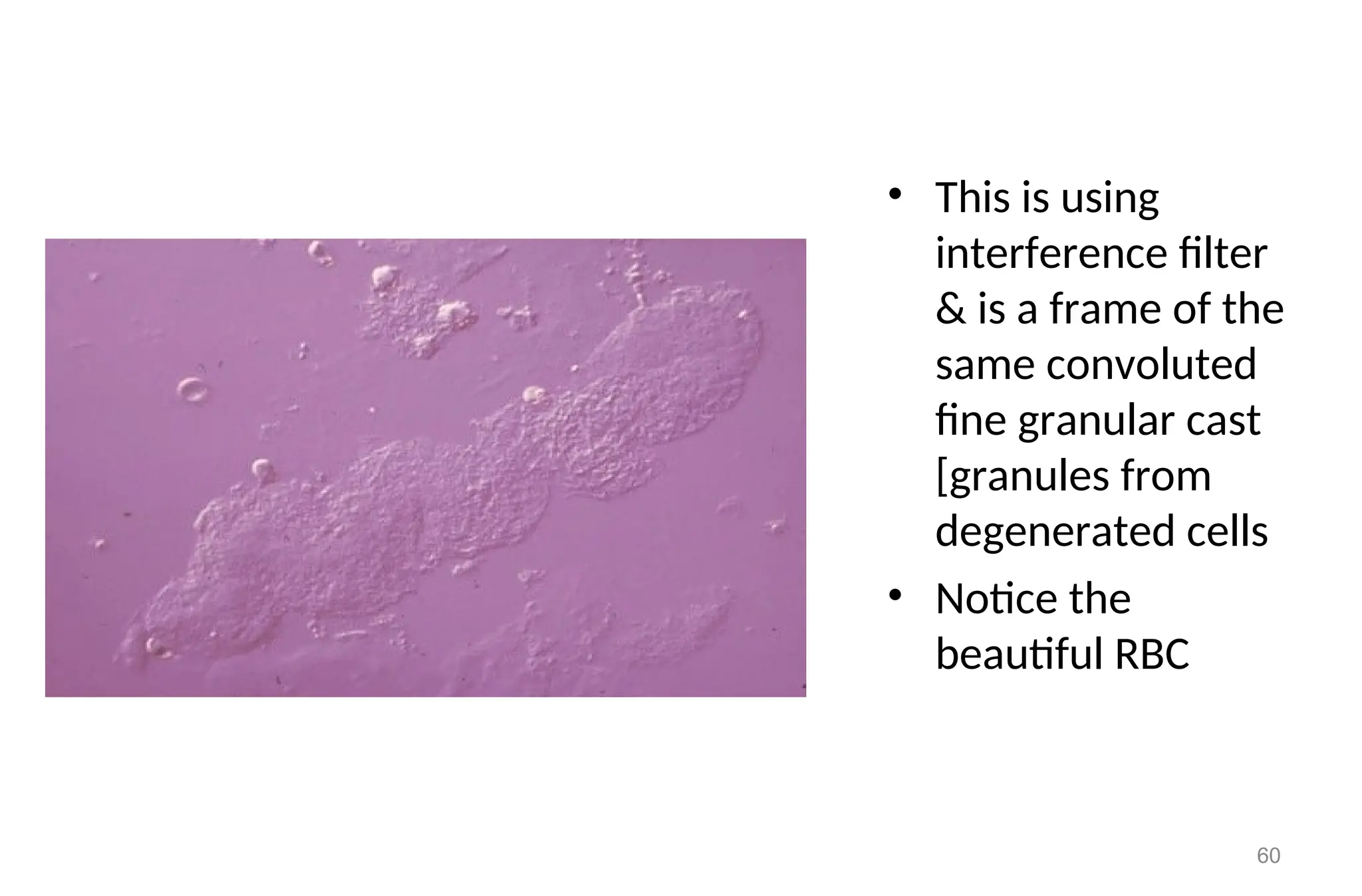
• This isusing
interference filter
& is a frame of the
same convoluted
fine granular cast
[granules from
degenerated cells
• Notice the
beautiful RBC
60
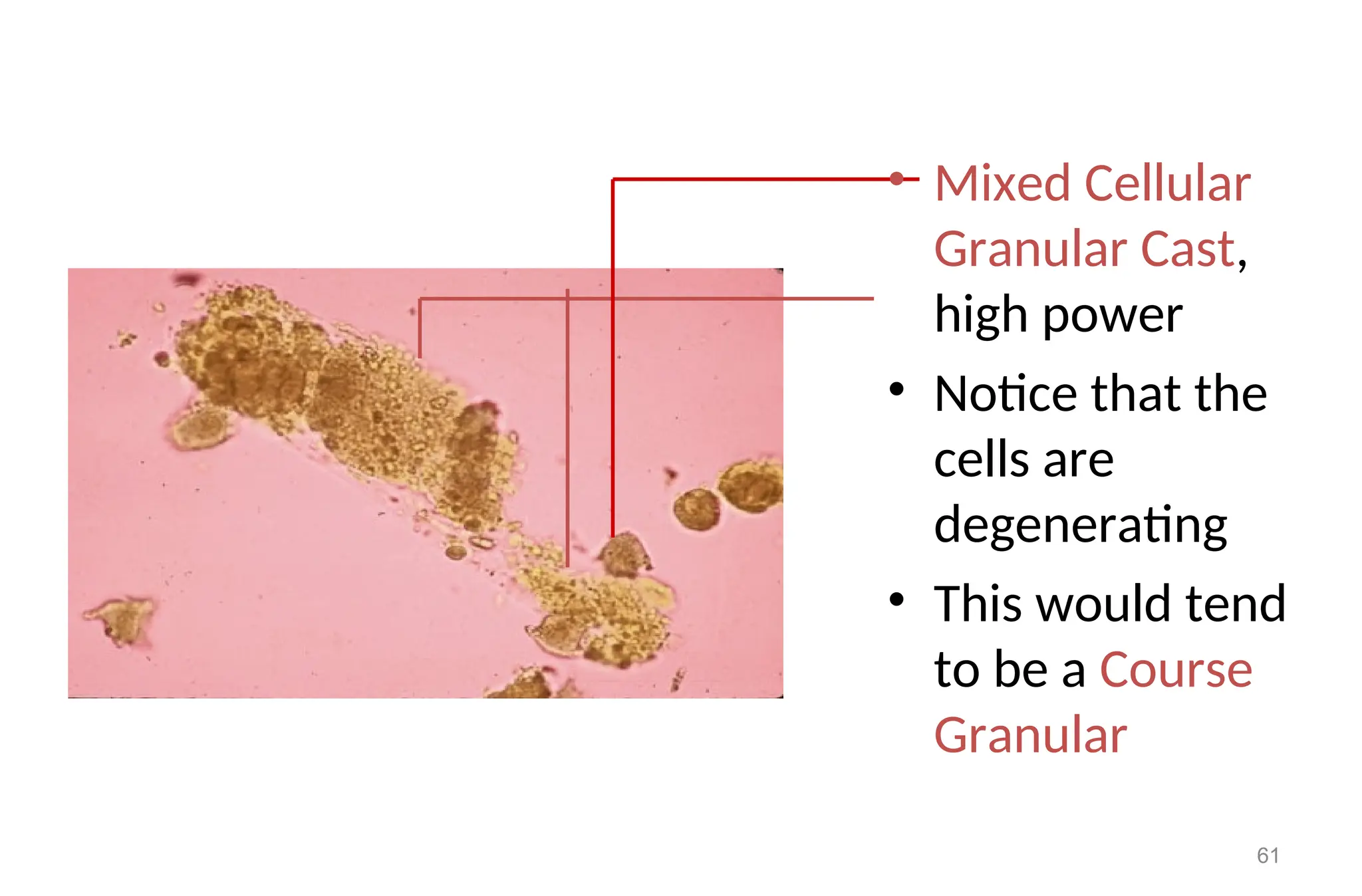
61.
• Mixed Cellular
GranularCast,
high power
• Notice that the
cells are
degenerating
• This would tend
to be a Course
Granular
61
Clinical significance
• Granularcasts may be seen in:
– Acute tubular necrosis
– Advanced granulonephritis
– Pyelonephrites
– Malignant nephrosis
– Chronic lead poisoning
– In healthy individuals these casts may be seen
– after strenuous exercise
66
67.
Cellular & OtherCast
• As the protein concentrates in the distal tubule & becomes
stickier, cells can become entrapped
• These become Hyaline Casts with Inclusions & while the
formal name would be for example Hyaline-WBC Cast, they
are frequently simply referred to as WBC Cast
67
68.
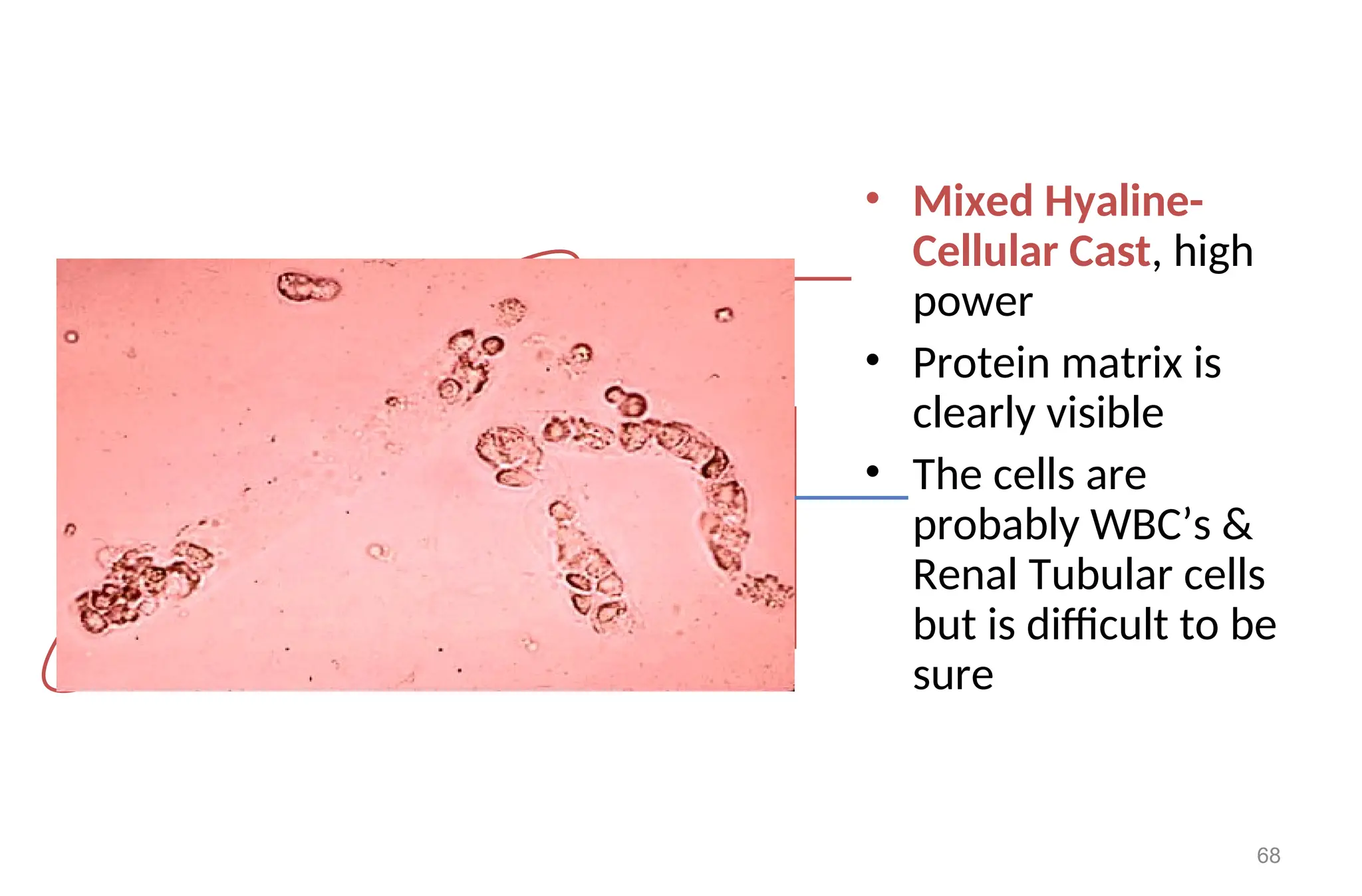
• Mixed Hyaline-
CellularCast, high
power
• Protein matrix is
clearly visible
• The cells are
probably WBC’s &
Renal Tubular cells
but is difficult to be
sure
68
69.
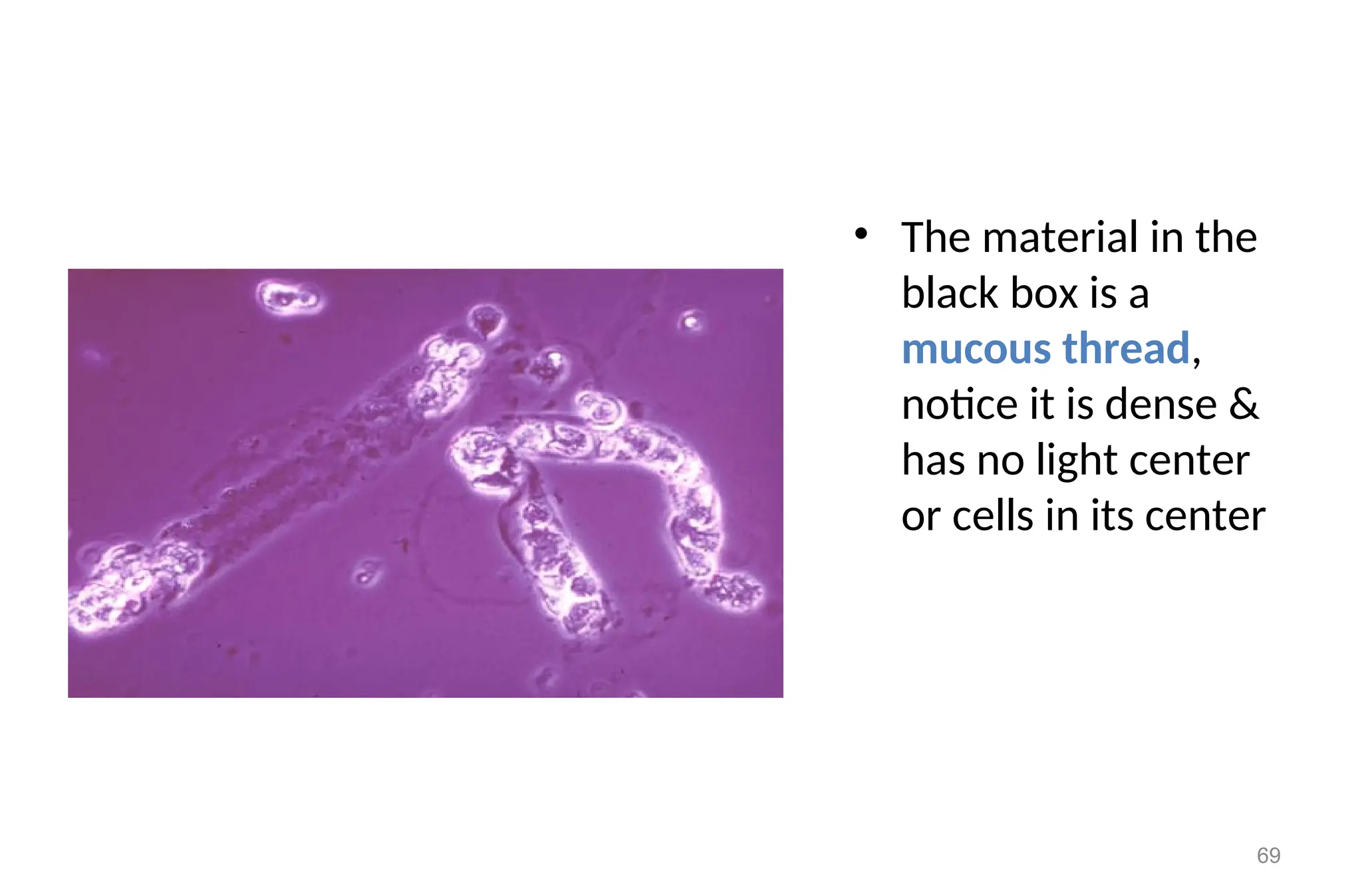
• The materialin the
black box is a
mucous thread,
notice it is dense &
has no light center
or cells in its center
69
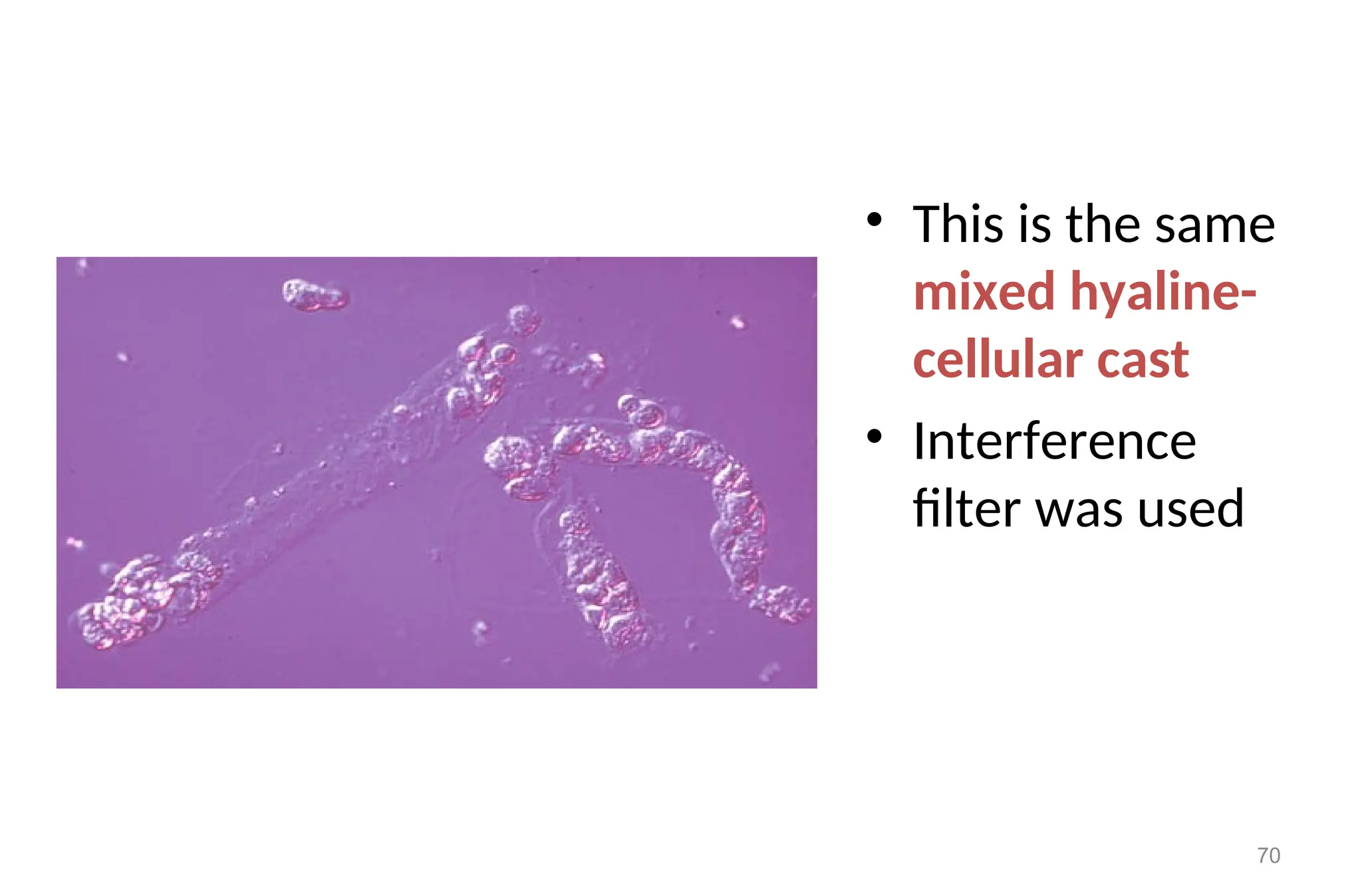
70.
• This isthe same
mixed hyaline-
cellular cast
• Interference
filter was used
70
71.
White blood cellcasts
formed by aggregates of white blood cells that
trapped in protein matrix in the renal tubular
lumen.
An excess of white blood cells, singly or in
clamps, in the urine may indicate inflammation.
white blood cell casts definitely are renal origin.
They characteristically seen in acute pyelonephrities and
occasionally in glomerulonephirites.
71
72.
Leukocyte Casts
• Upperurinary tract
• inflammation of the kidney
• pyelonephritis
• Interstitial nephritis
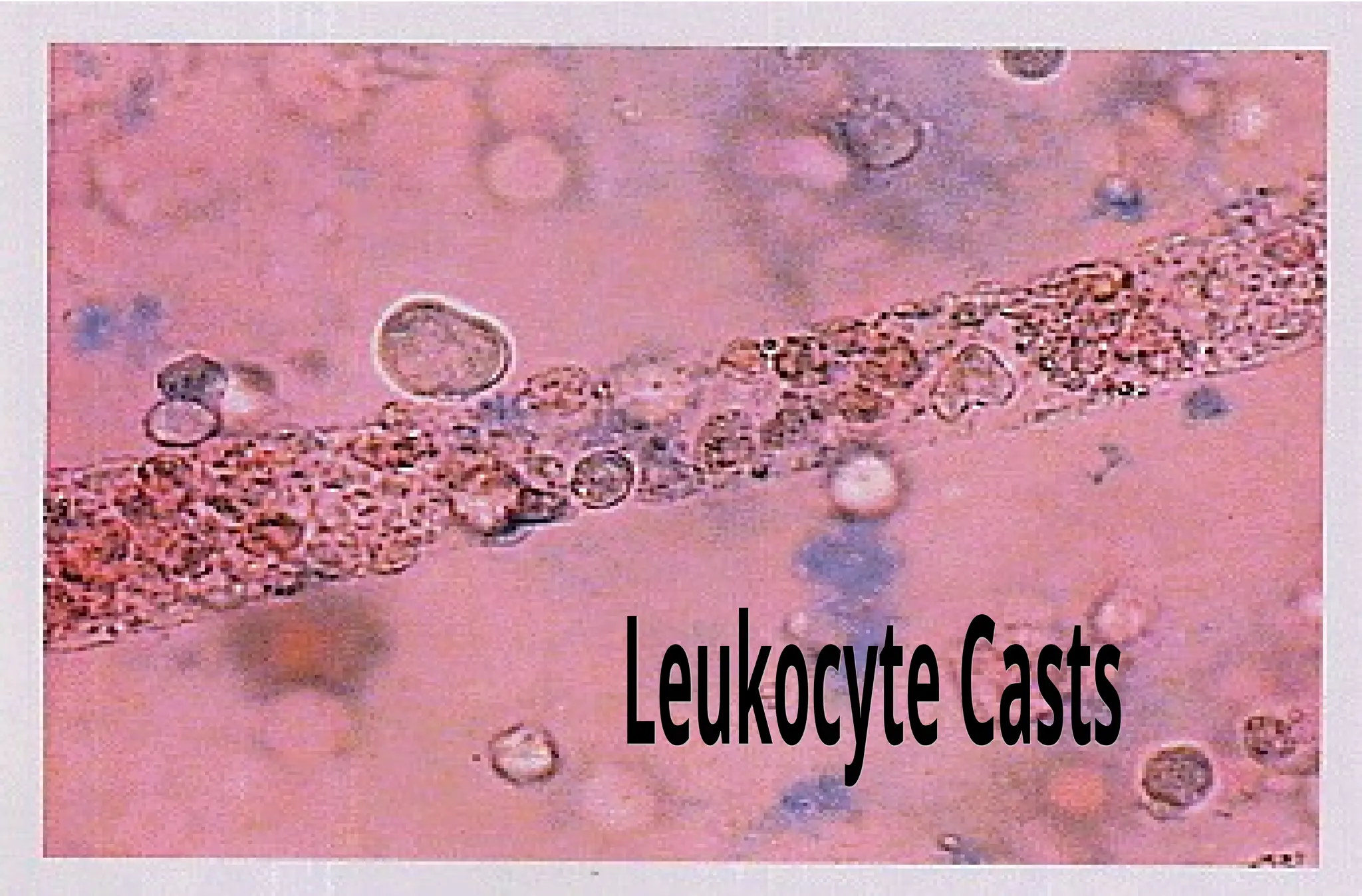
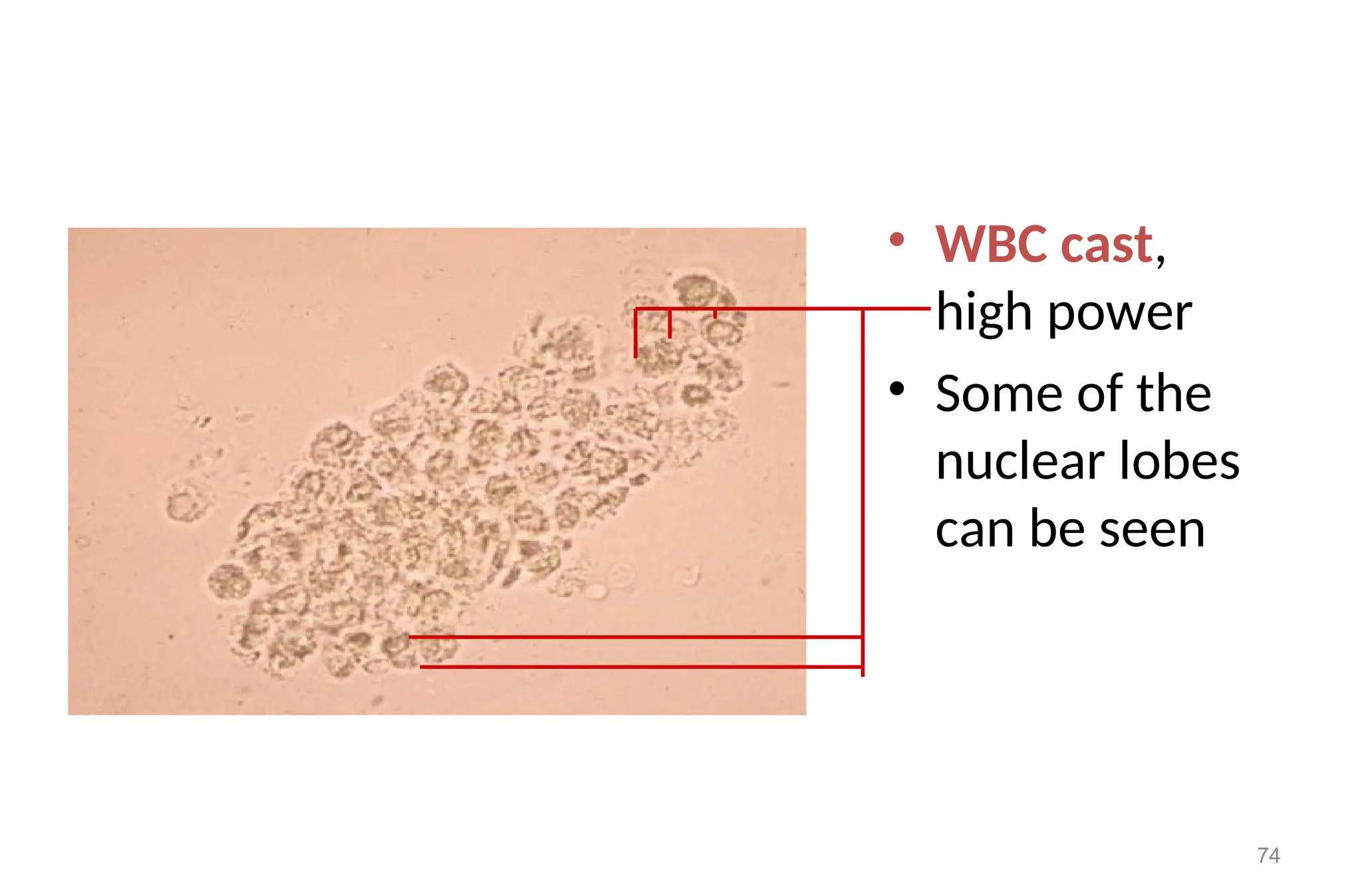
74.
• WBC cast,
highpower
• Some of the
nuclear lobes
can be seen
74
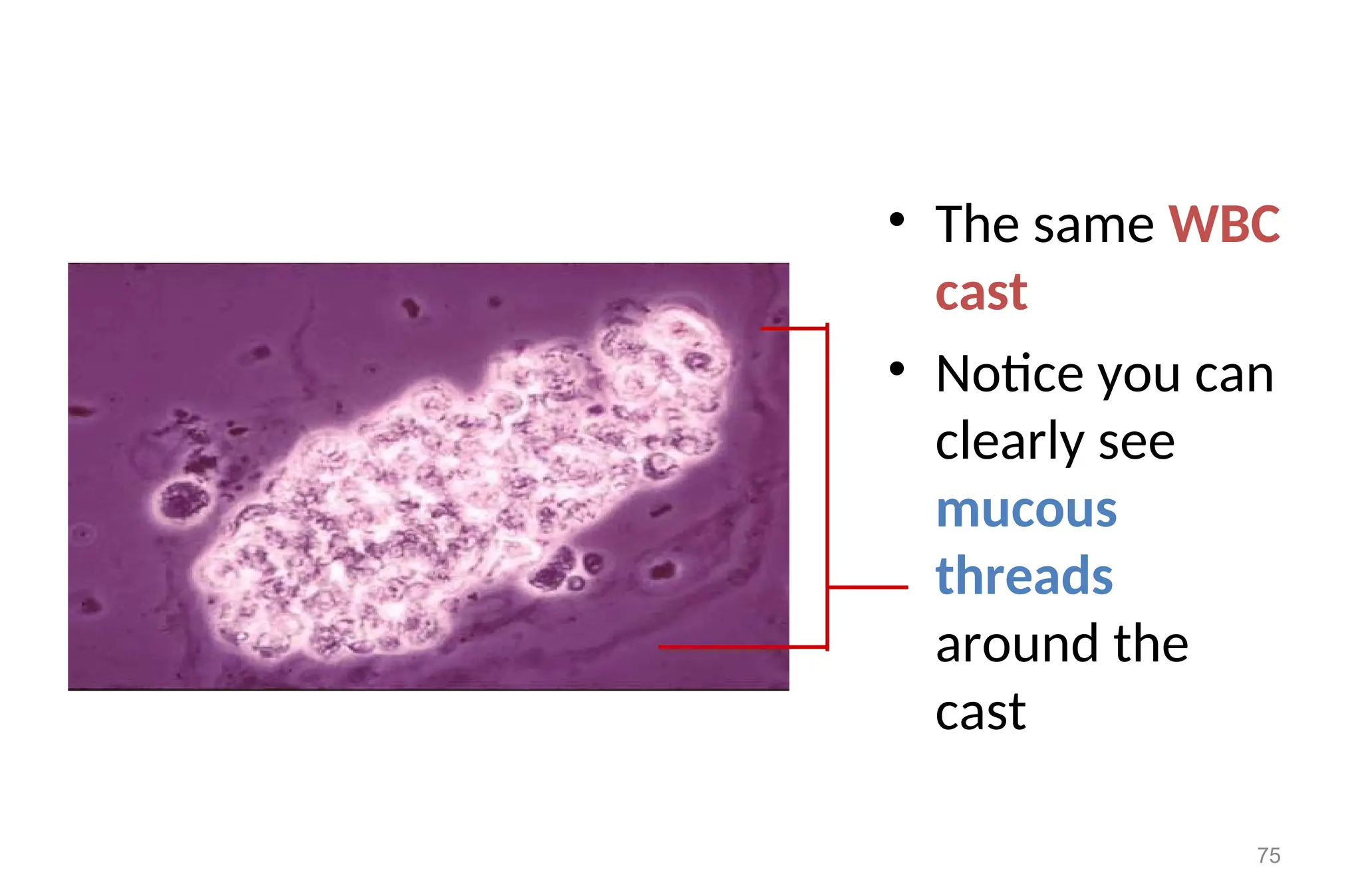
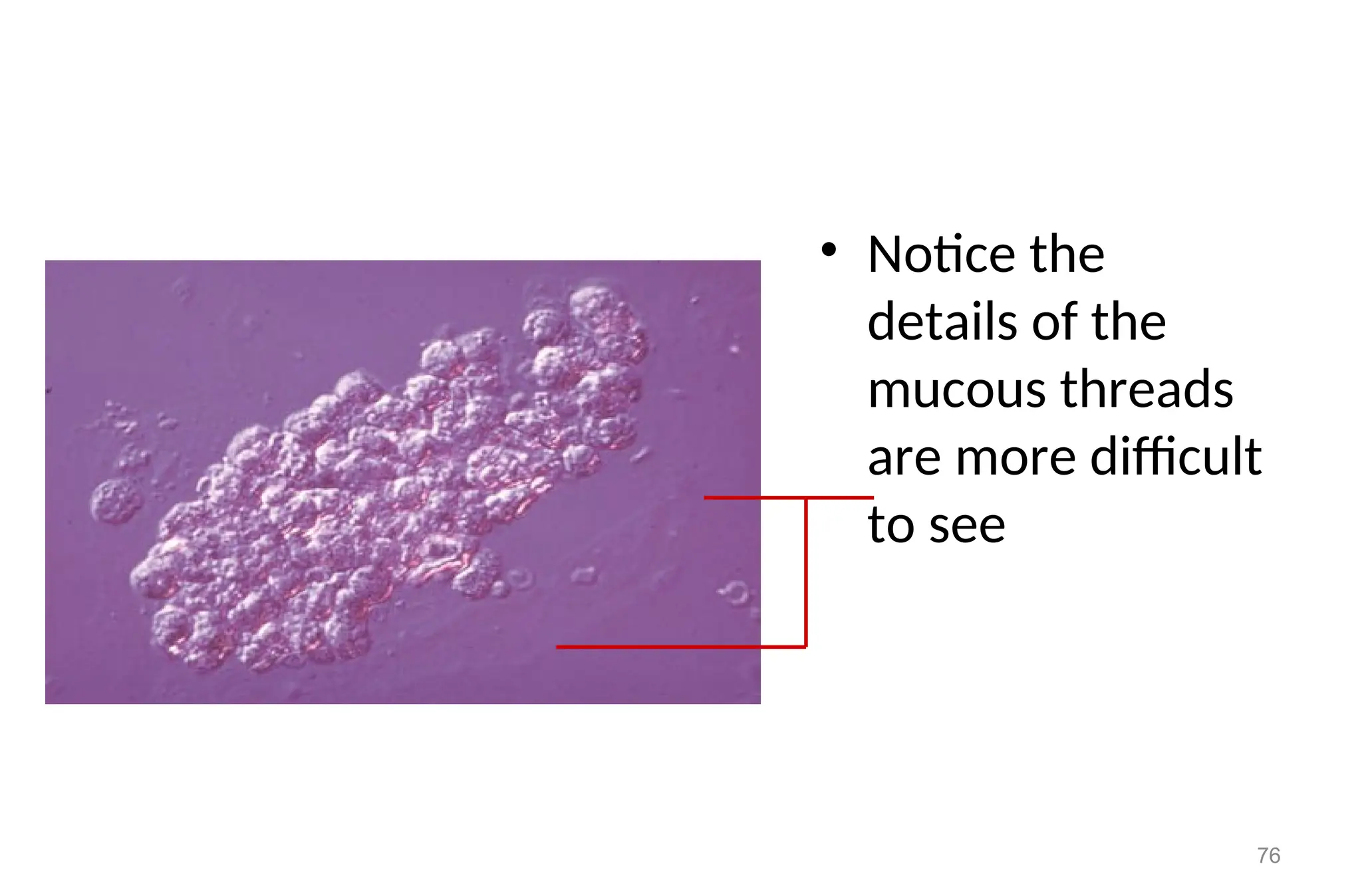
75.
• The sameWBC
cast
• Notice you can
clearly see
mucous
threads
around the
cast
75
Red blood cellcasts
- Usually, they found in hematuria. Red blood cell casts may
appear broen to almost colorless and are usually diagnostic of
glomerular diseases.
- Normal range: normally not seen in normal individual
- Appearance
- Formed usually after accumulation of cellular element in the
renal tubules
77
78.
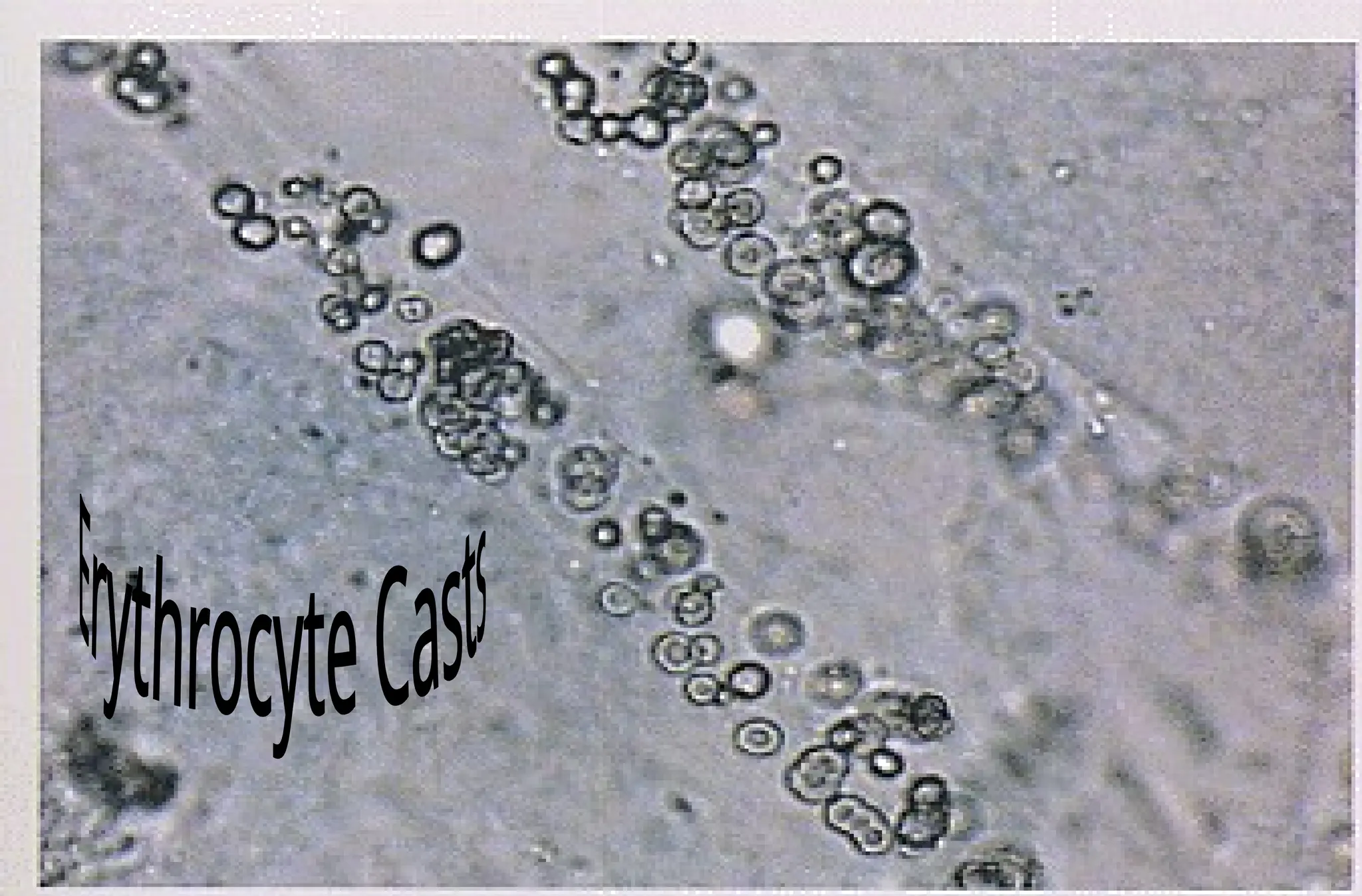
Erythrocyte Casts
• indicateglomerulonephritis
• Primary glomerular disease with RBC’s passing the damaged
glomeruli in large quantities
• Lupus nephritis
• rapidly progressive glomerulonephritis
79.
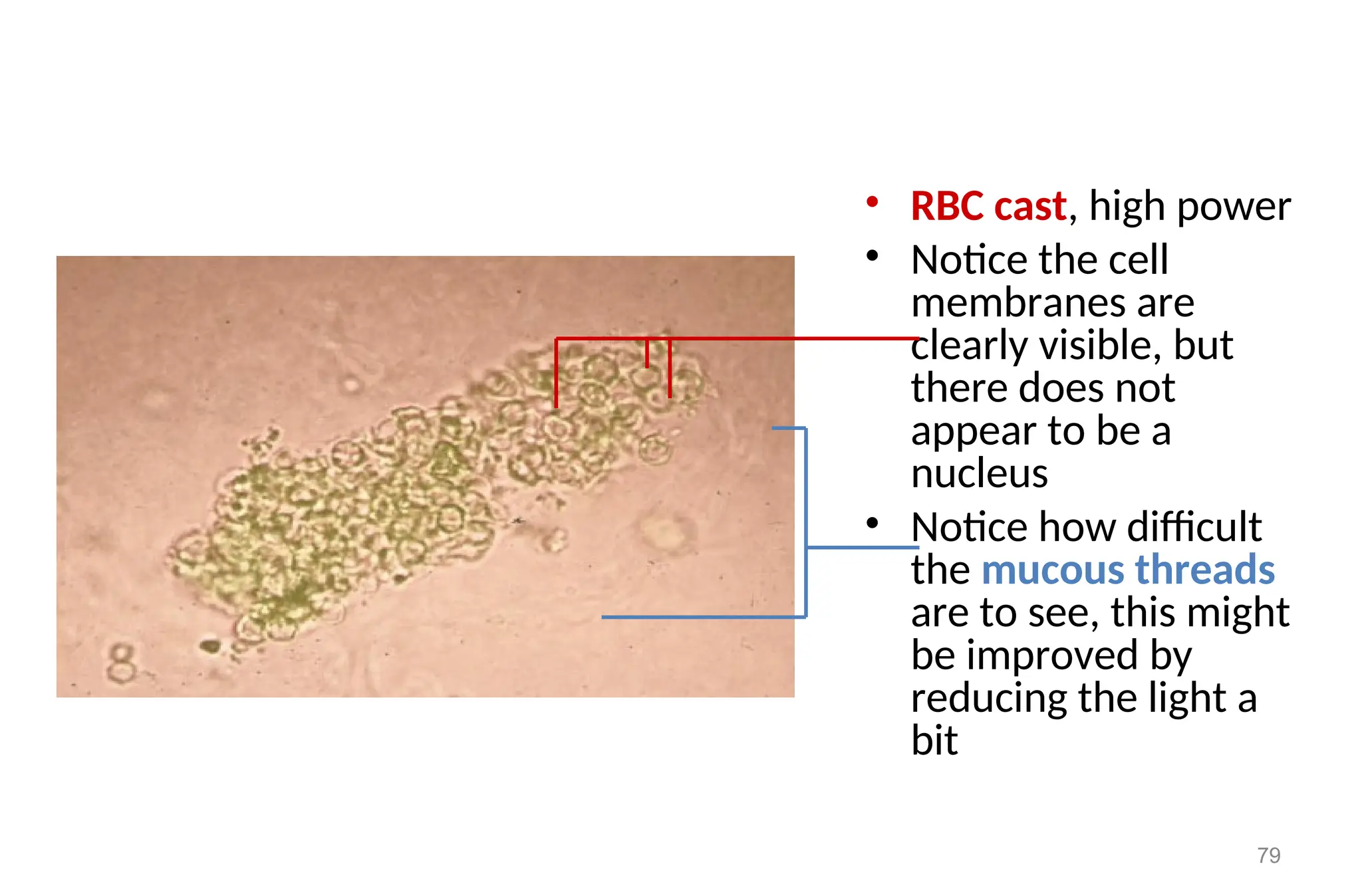
• RBC cast,high power
• Notice the cell
membranes are
clearly visible, but
there does not
appear to be a
nucleus
• Notice how difficult
the mucous threads
are to see, this might
be improved by
reducing the light a
bit
79
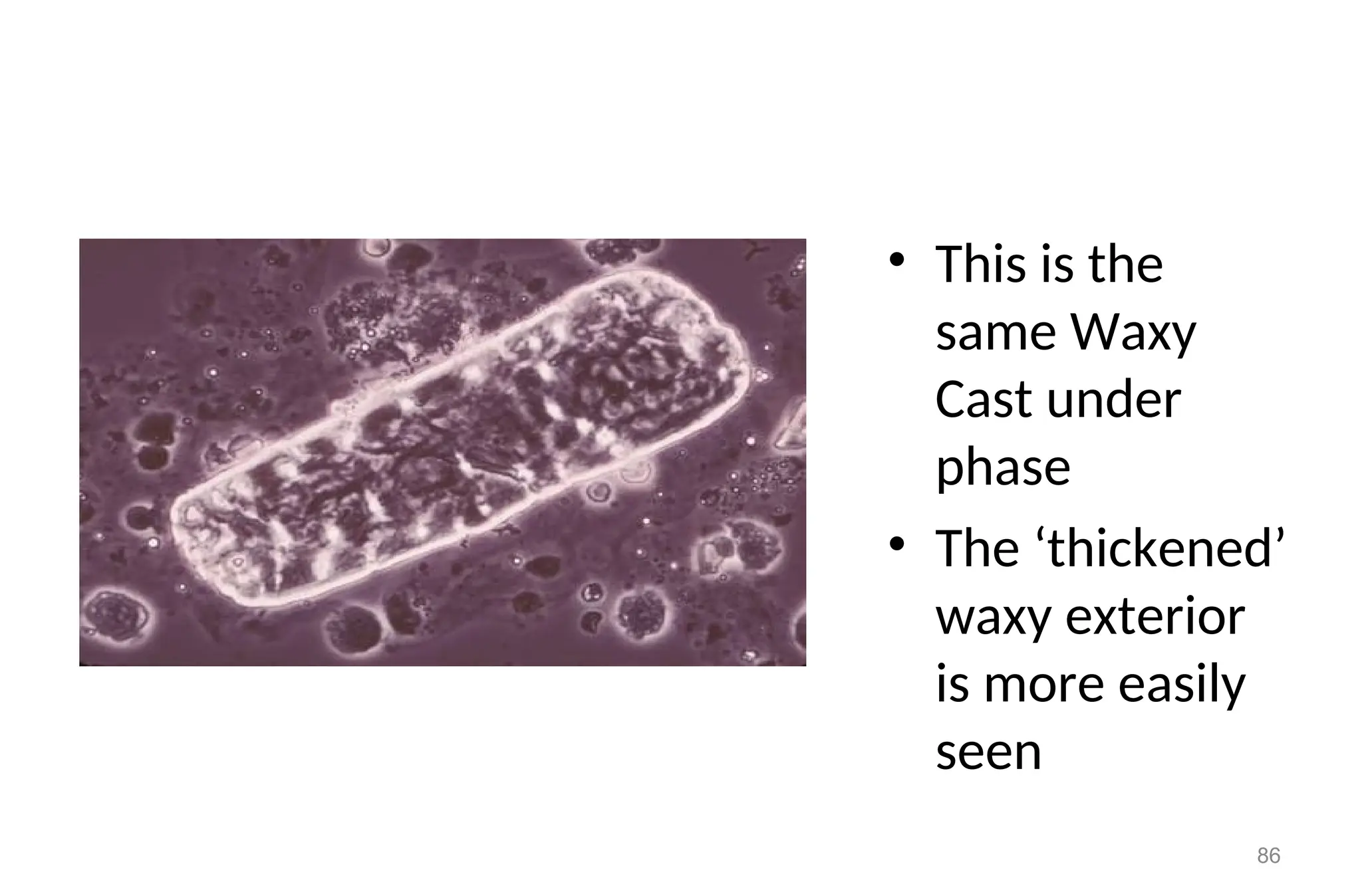
81.
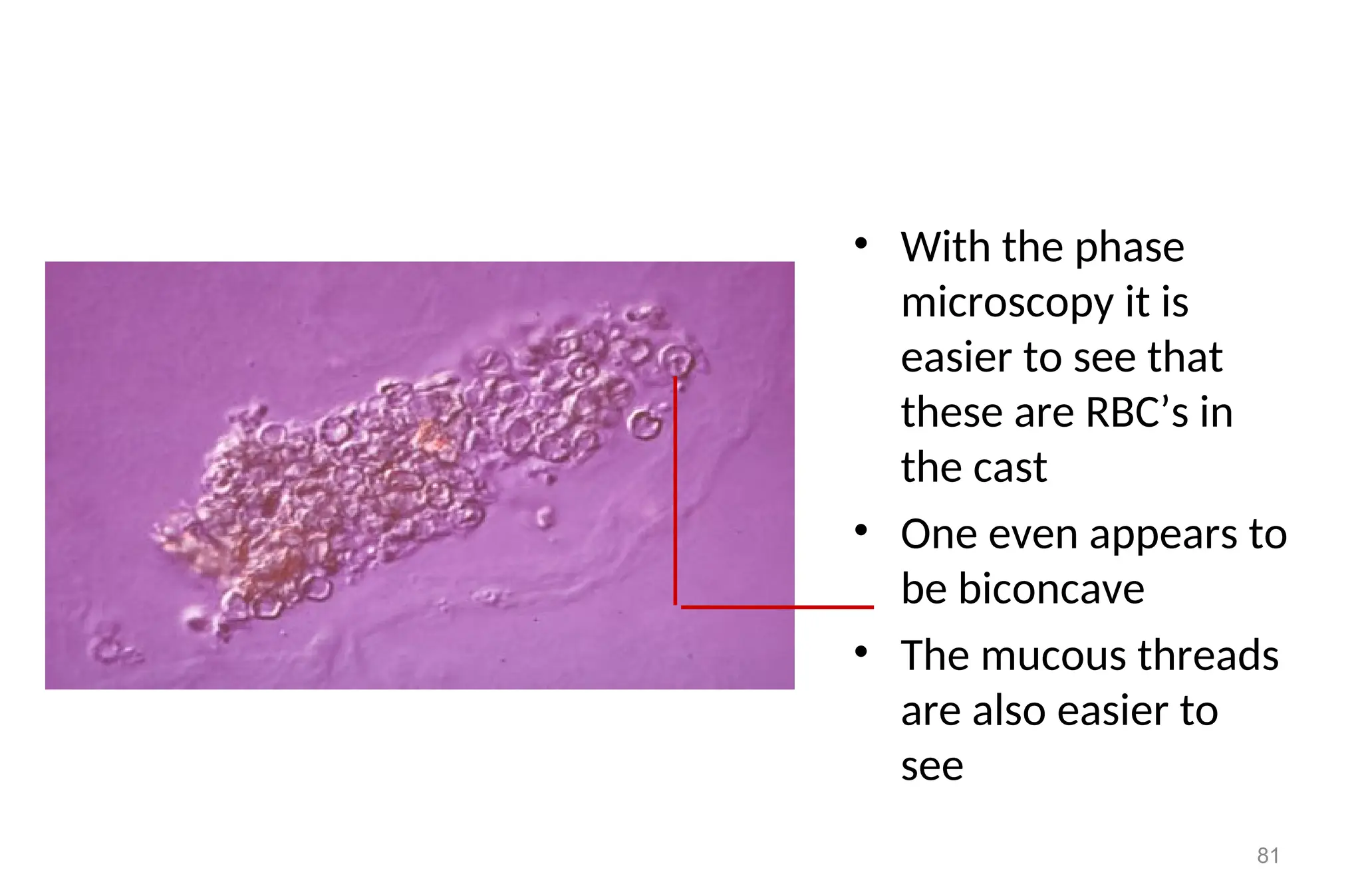
• With thephase
microscopy it is
easier to see that
these are RBC’s in
the cast
• One even appears to
be biconcave
• The mucous threads
are also easier to
see
81
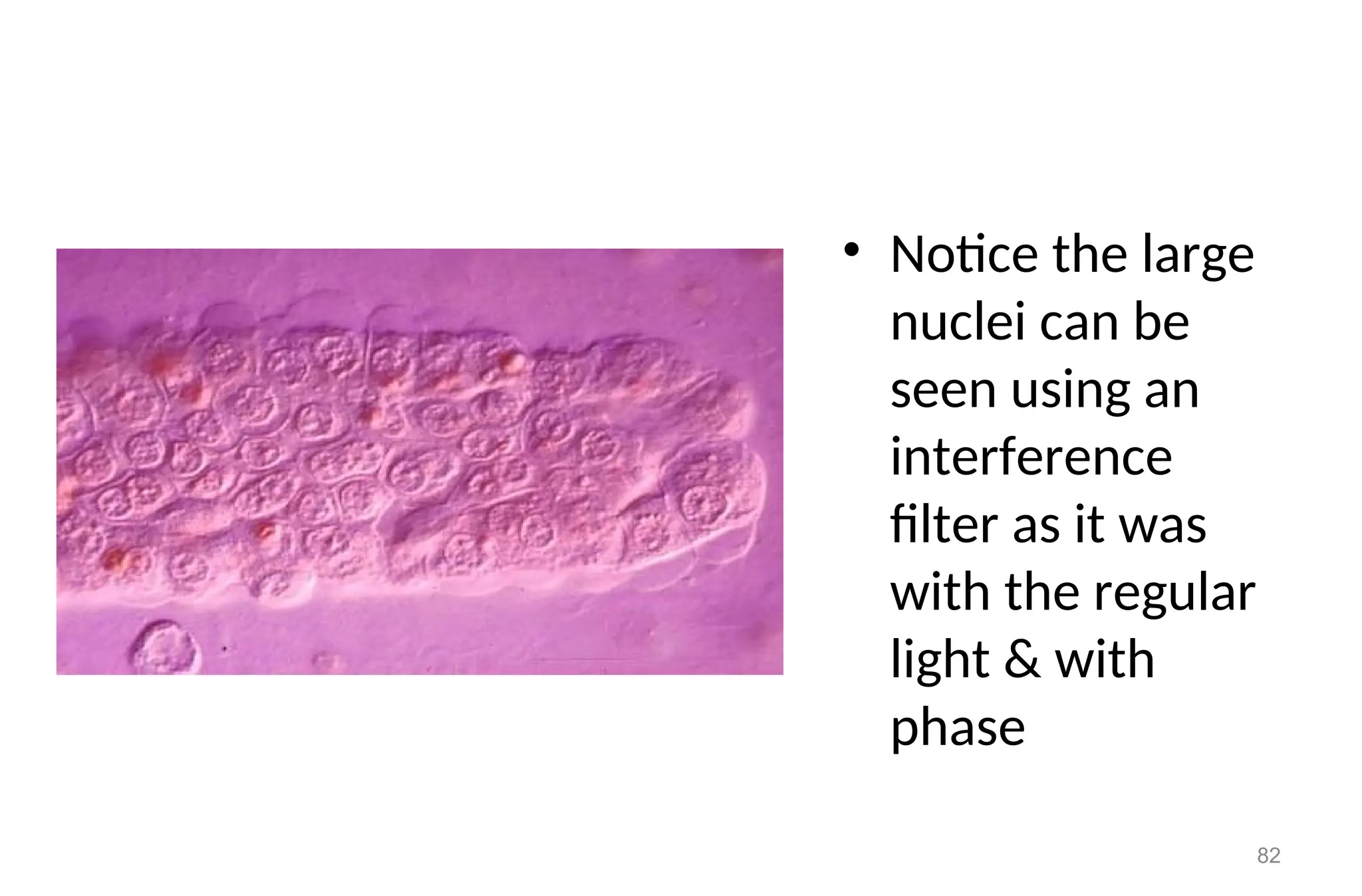
82.
• Notice thelarge
nuclei can be
seen using an
interference
filter as it was
with the regular
light & with
phase
82
83.
Waxy Casts (RenalFailure Casts)
• Not seen in normal individuals.
• Appearance
• Shorter and broader than hyaline casts.
• Composed of homogeneous, yellowish materials.
• Broad waxy casts are from two to six times the width of ordinary
• appear waxy and granular.
• Have high retractive index.
• May occur from cells (WBC, RBC, or Epithelial) casts, hyaline
casts.
83
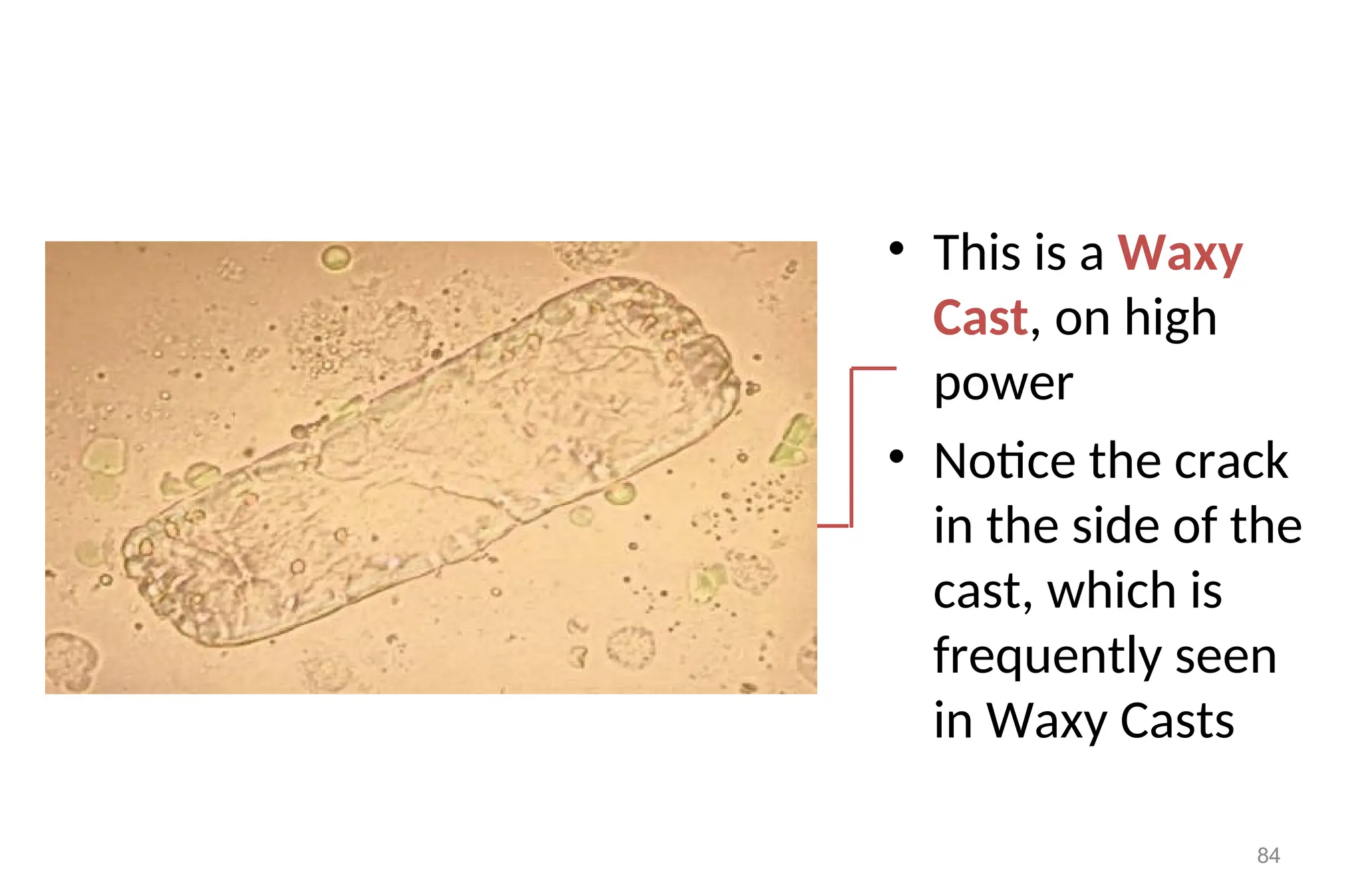
84.
• This isa Waxy
Cast, on high
power
• Notice the crack
in the side of the
cast, which is
frequently seen
in Waxy Casts
84
Waxy Casts
Clinical significance
•Waxy casts are found in
• Chronic renal disease.
• Tubular inflammation and degeneration.
• Localized nephron obstruction.
• malignant hypertension
• in diabetic diseases (nephropathy)
• The presence of waxy casts indicates severity of renal disease.
88
89.
Fatty Casts
normallynot seen in health individuals.
Appearance:
These are casts, which contain fat droplets inside them.
Fat droplets are formed after accumulation of fat in the tubular
vessels, especially tubular epithelial and finally disintegrated.
Clinical Implication:
The occurrence of fat droplets, oval, fat bodies, or fat casts is
very important sign of nephritic syndrome.
Chronic renal disease.
Inflammation and degeneration of renal tubules.
lupus and toxic renal poisoning
89
90.
• This isa cast
containing ‘fat’
bodies, high
power
• On wet mount the
droplets are
highly refractile
[they bounce the
light back]
90
91.
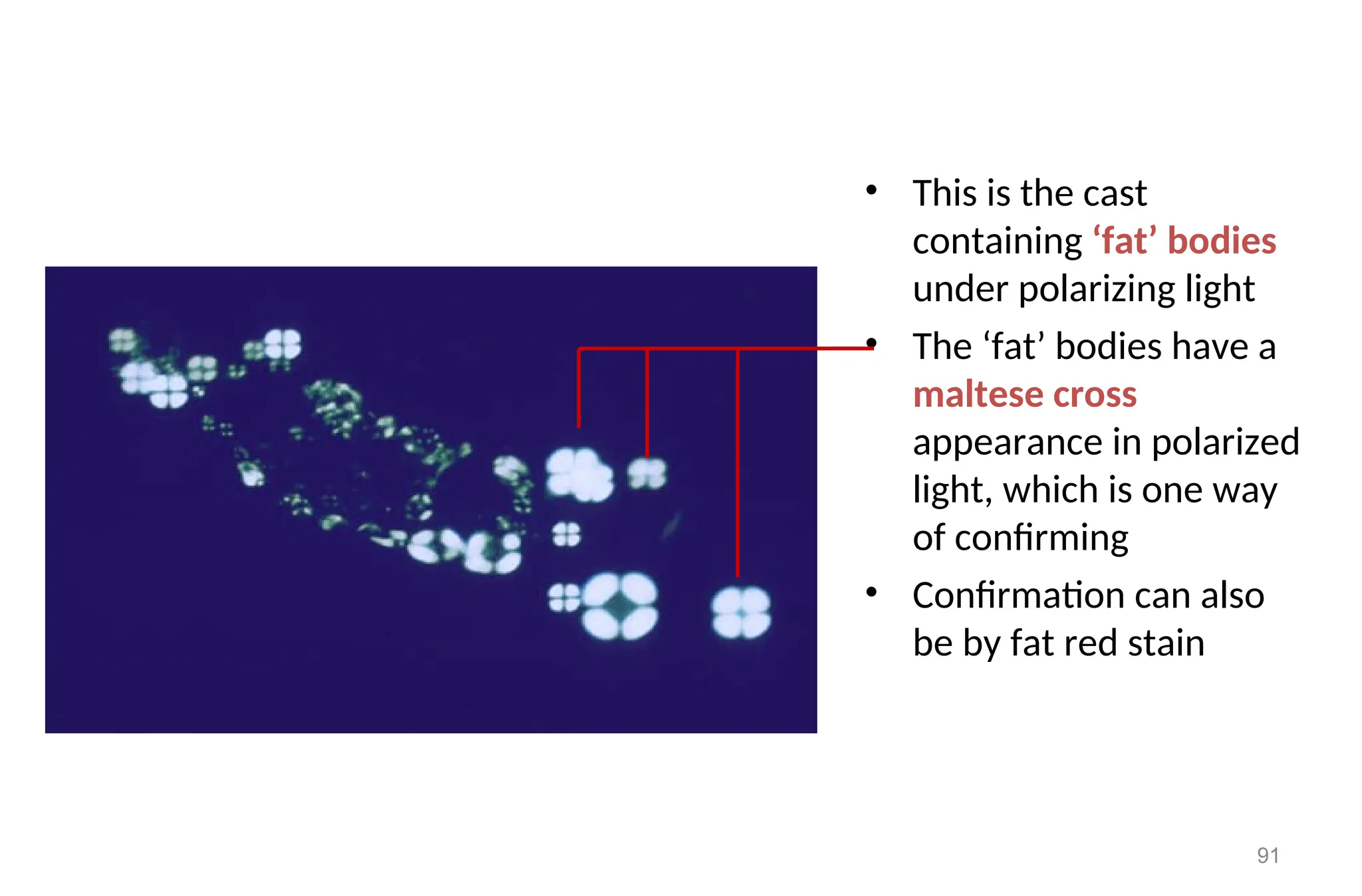
• This isthe cast
containing ‘fat’ bodies
under polarizing light
• The ‘fat’ bodies have a
maltese cross
appearance in polarized
light, which is one way
of confirming
• Confirmation can also
be by fat red stain
91
92.
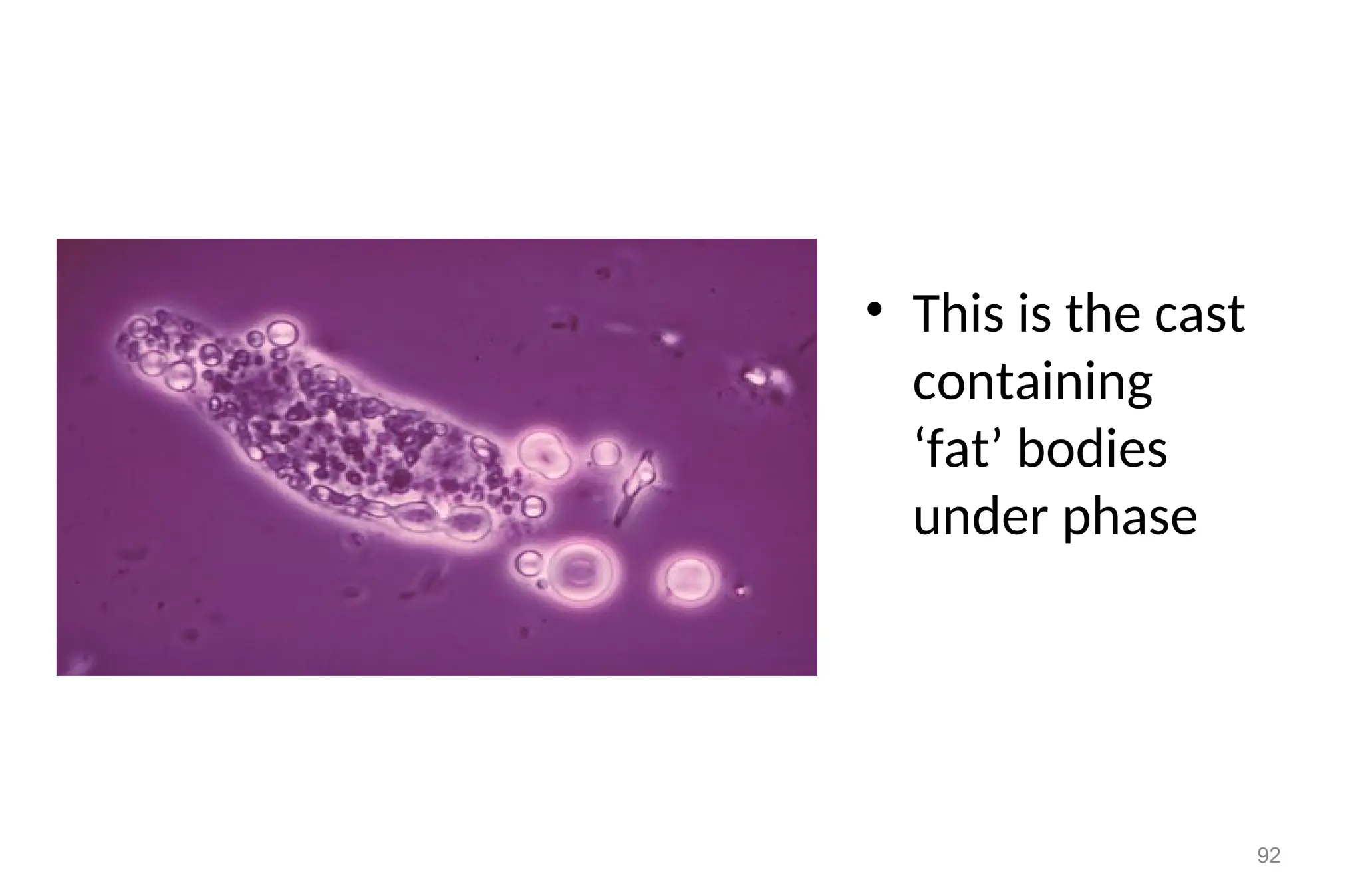
• This isthe cast
containing
‘fat’ bodies
under phase
92
93.
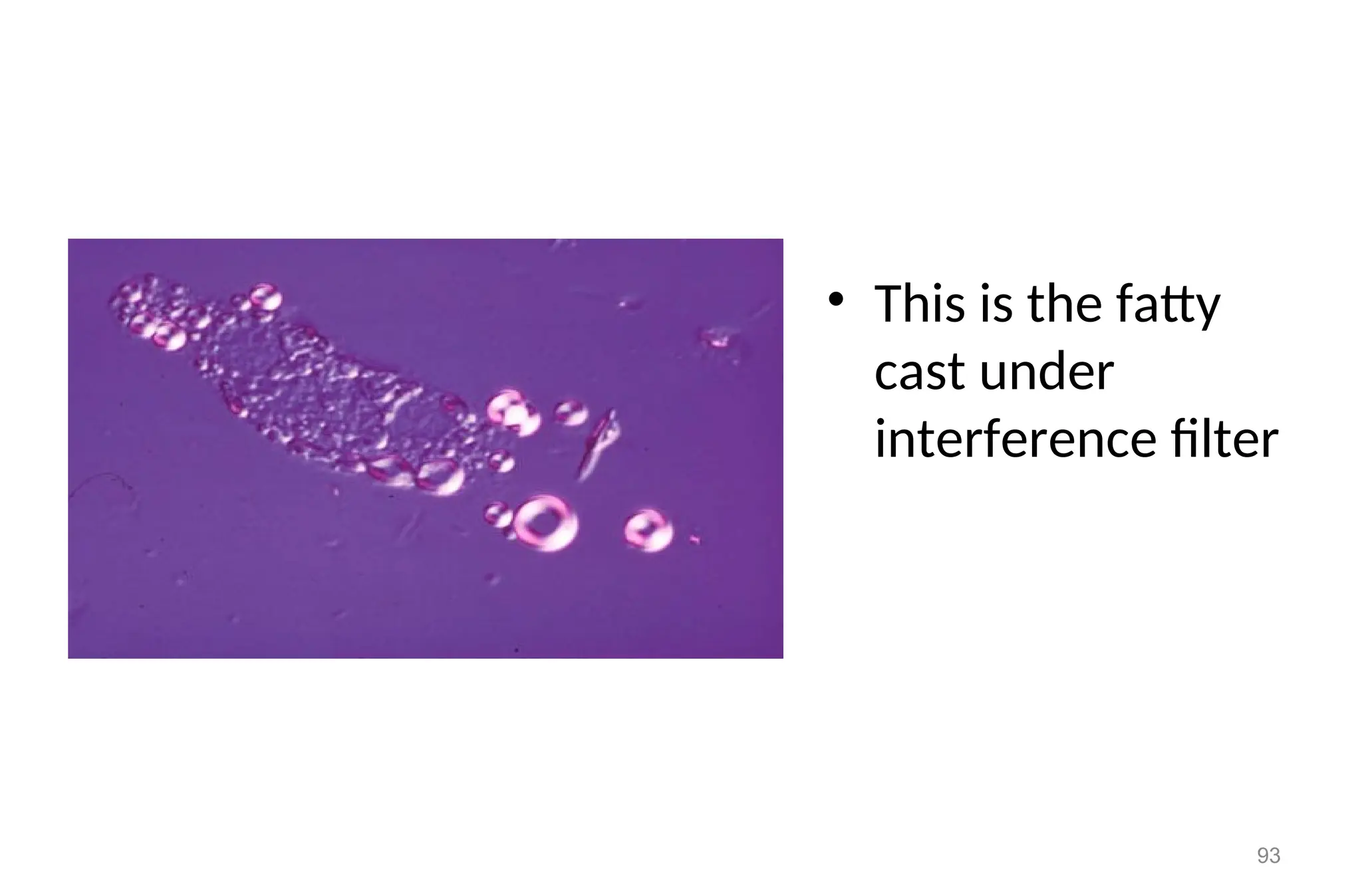
• This isthe fatty
cast under
interference filter
93
94.
Epithelial Casts
• EpithelialCasts are composed largely of tubular epithelial cell
desquamated within the tubule.
• They often appear as two rows if cells in protein cast matrix.
• Inflammation of the kidney may cause greater sloughing of renal
epithelial cells, so large number of epithelial casts is indicative of
renal parenchymal disease with tubular damage.
94
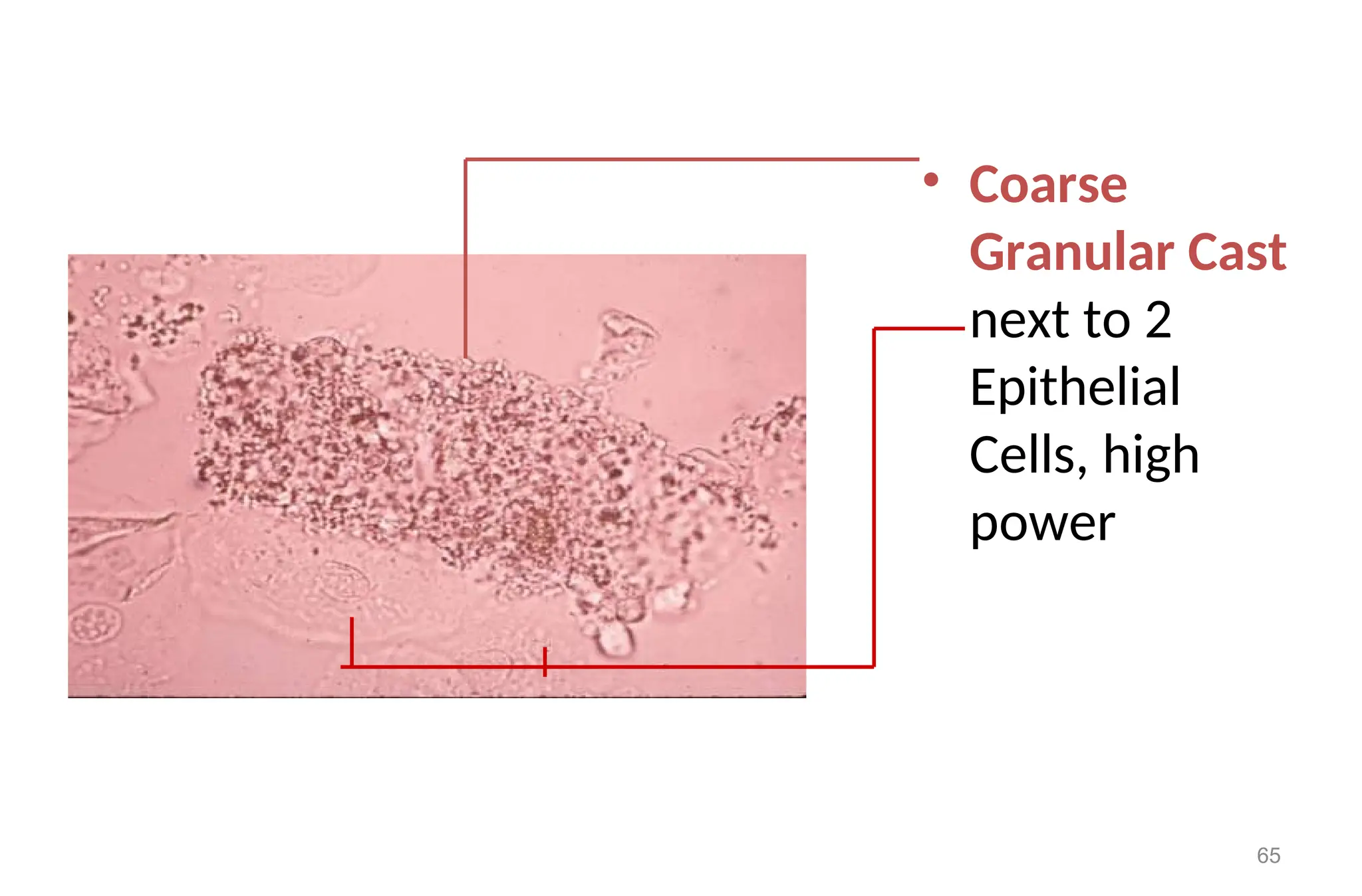
96.
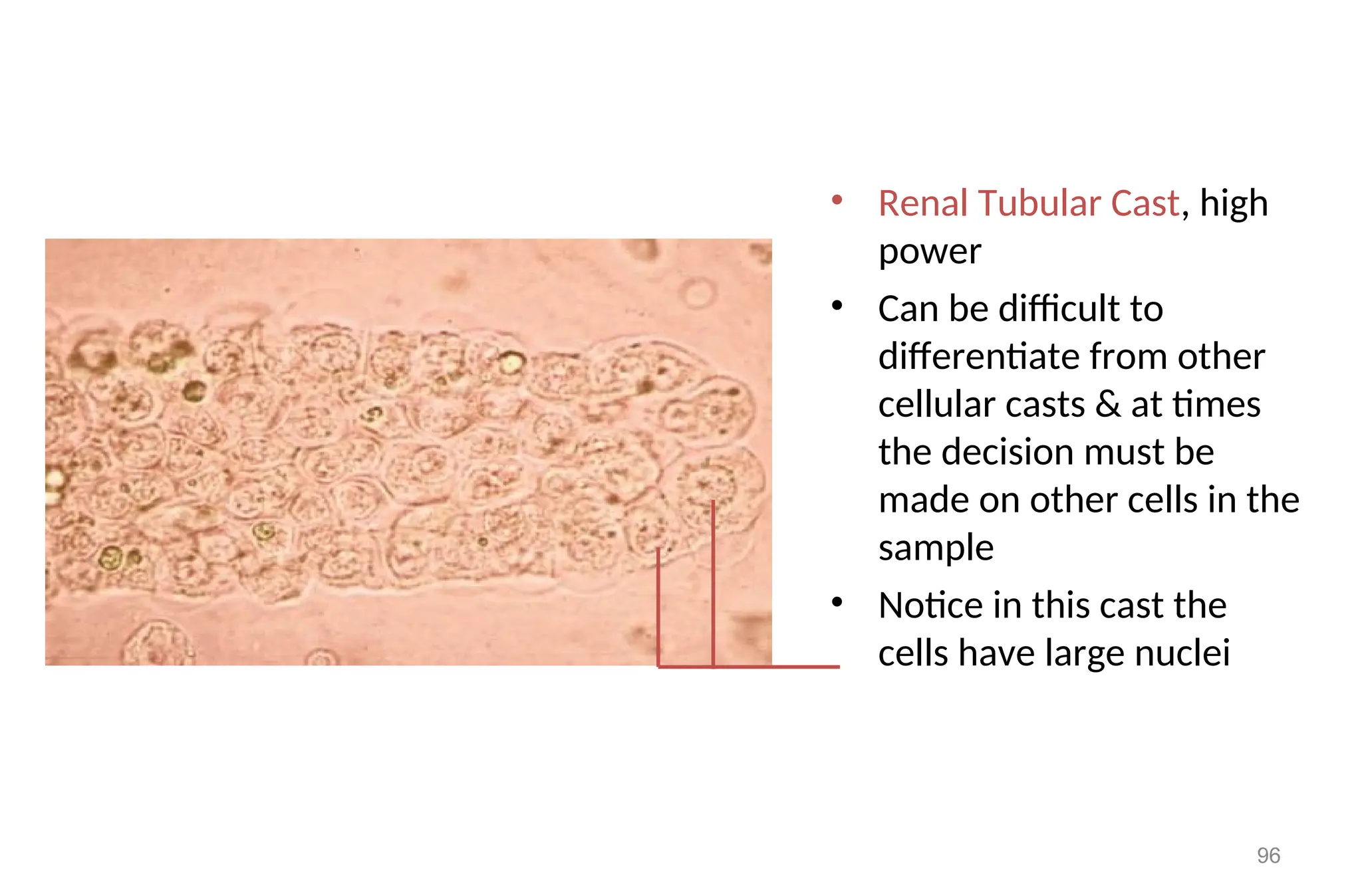
• Renal TubularCast, high
power
• Can be difficult to
differentiate from other
cellular casts & at times
the decision must be
made on other cells in the
sample
• Notice in this cast the
cells have large nuclei
96
98.
Reporting of casts
•Casts are examined under 10x objective of the microscope.
• Casts are reported quantitatively by saying:
– Few casts / LPF
– Moderate casts / LPF and
– Many casts / LPF
• During the report the, type of cast that is seen should also be
mentioned
• Example: few hyaline casts / LPF are seen
98
99.
PARASITES
• Parasites thatcan be seen in urine microscopy are:
• Trichomonas vaginalis
• Schistosoma haematobium
• Wuchereria bancroftie
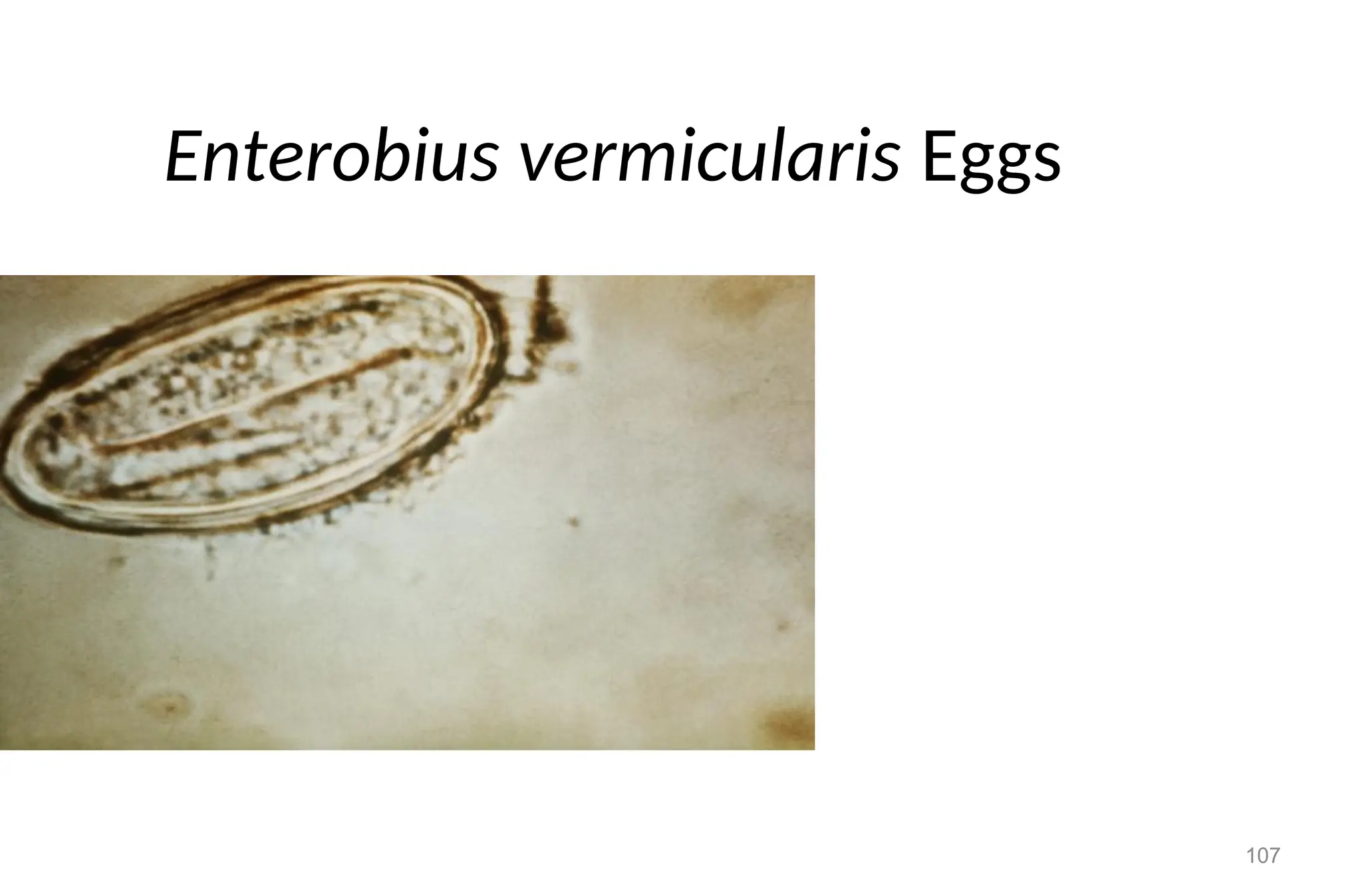
• Other parasites such as Entrobious vermicularies also may
occur due to contamination of the urine with stool.
99
100.
100
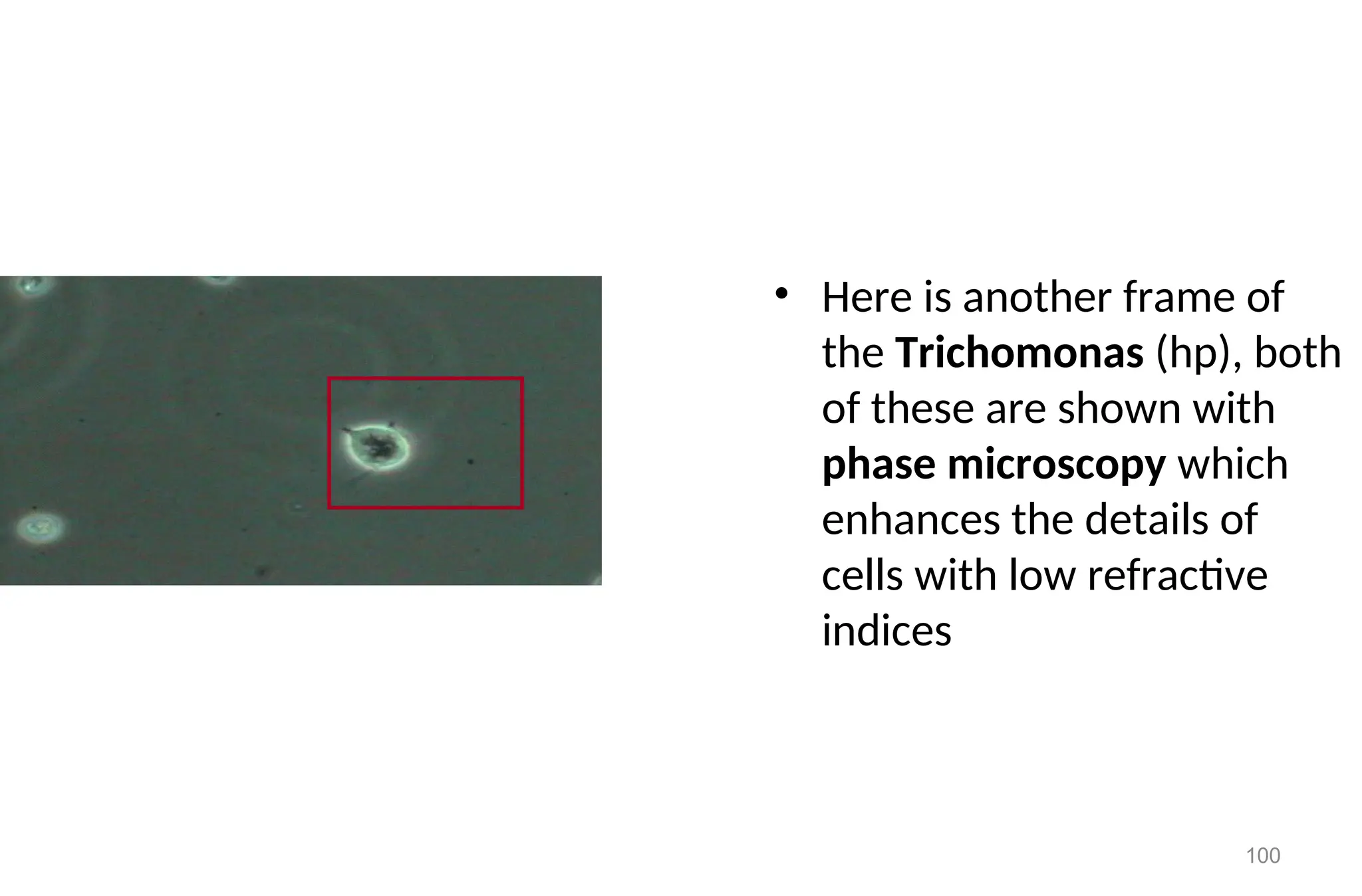
• Here isanother frame of
the Trichomonas (hp), both
of these are shown with
phase microscopy which
enhances the details of
cells with low refractive
indices
102
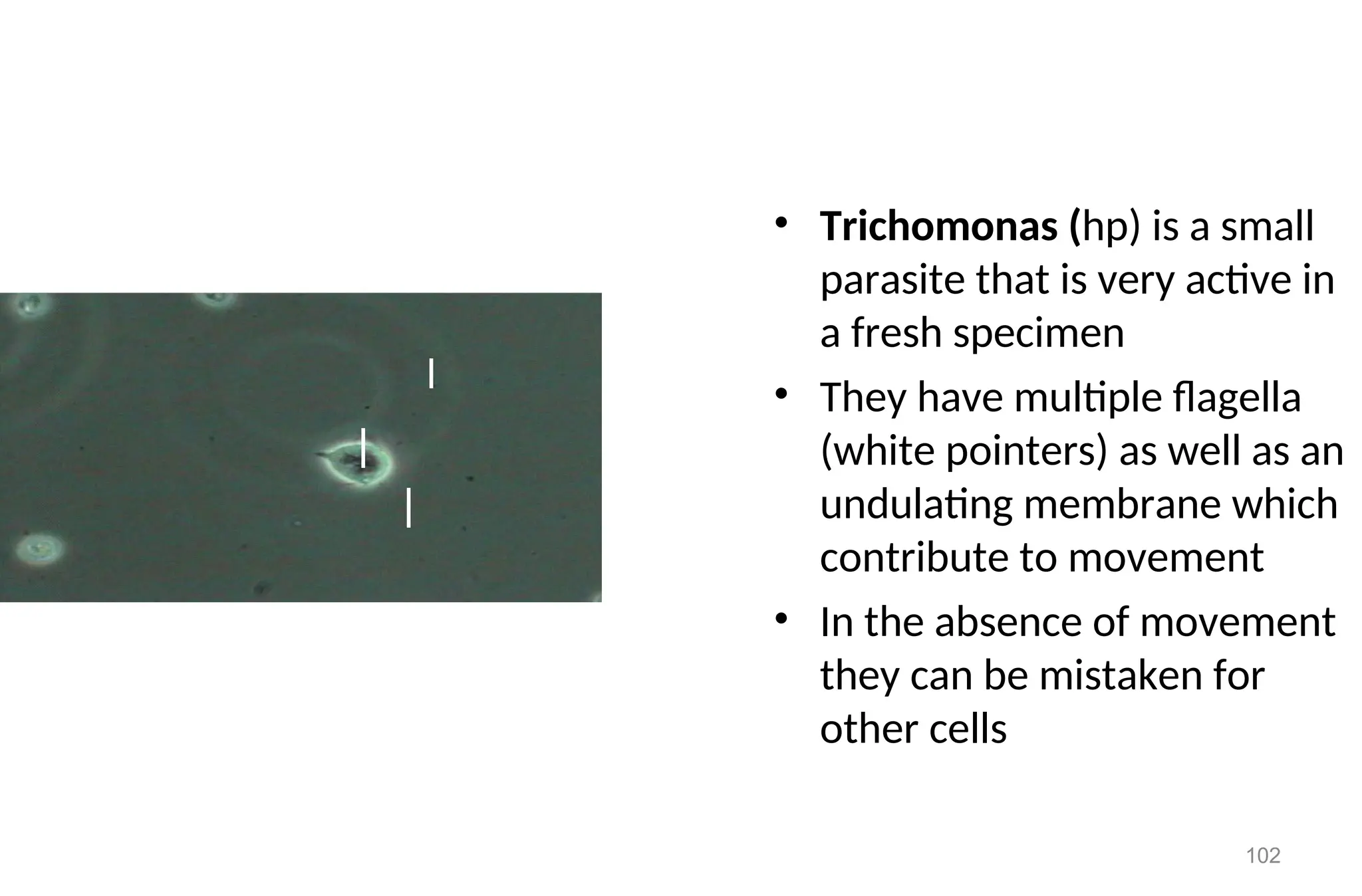
• Trichomonas (hp)is a small
parasite that is very active in
a fresh specimen
• They have multiple flagella
(white pointers) as well as an
undulating membrane which
contribute to movement
• In the absence of movement
they can be mistaken for
other cells
103.
103
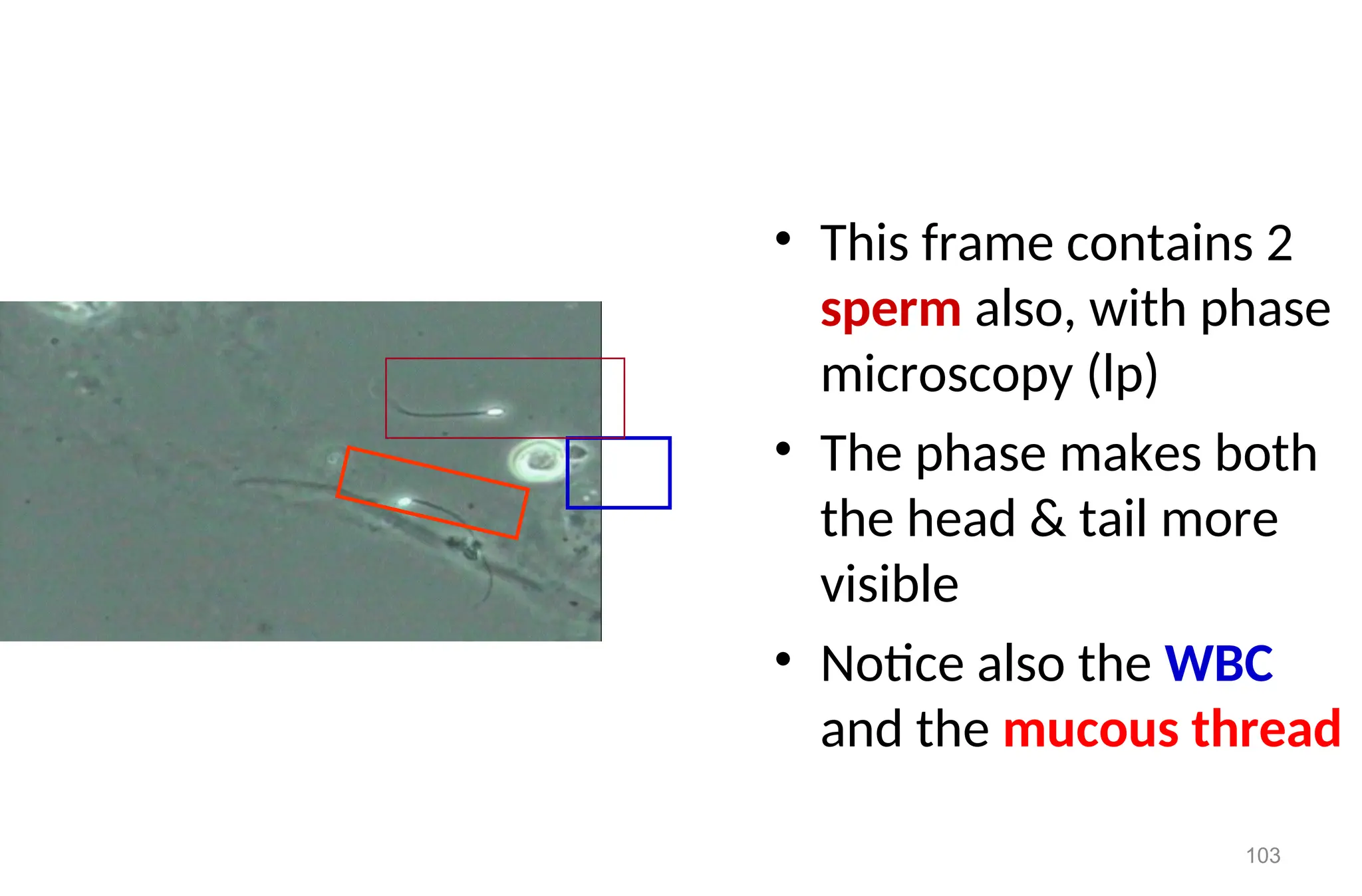
• This framecontains 2
sperm also, with phase
microscopy (lp)
• The phase makes both
the head & tail more
visible
• Notice also the WBC
and the mucous thread
104.
104
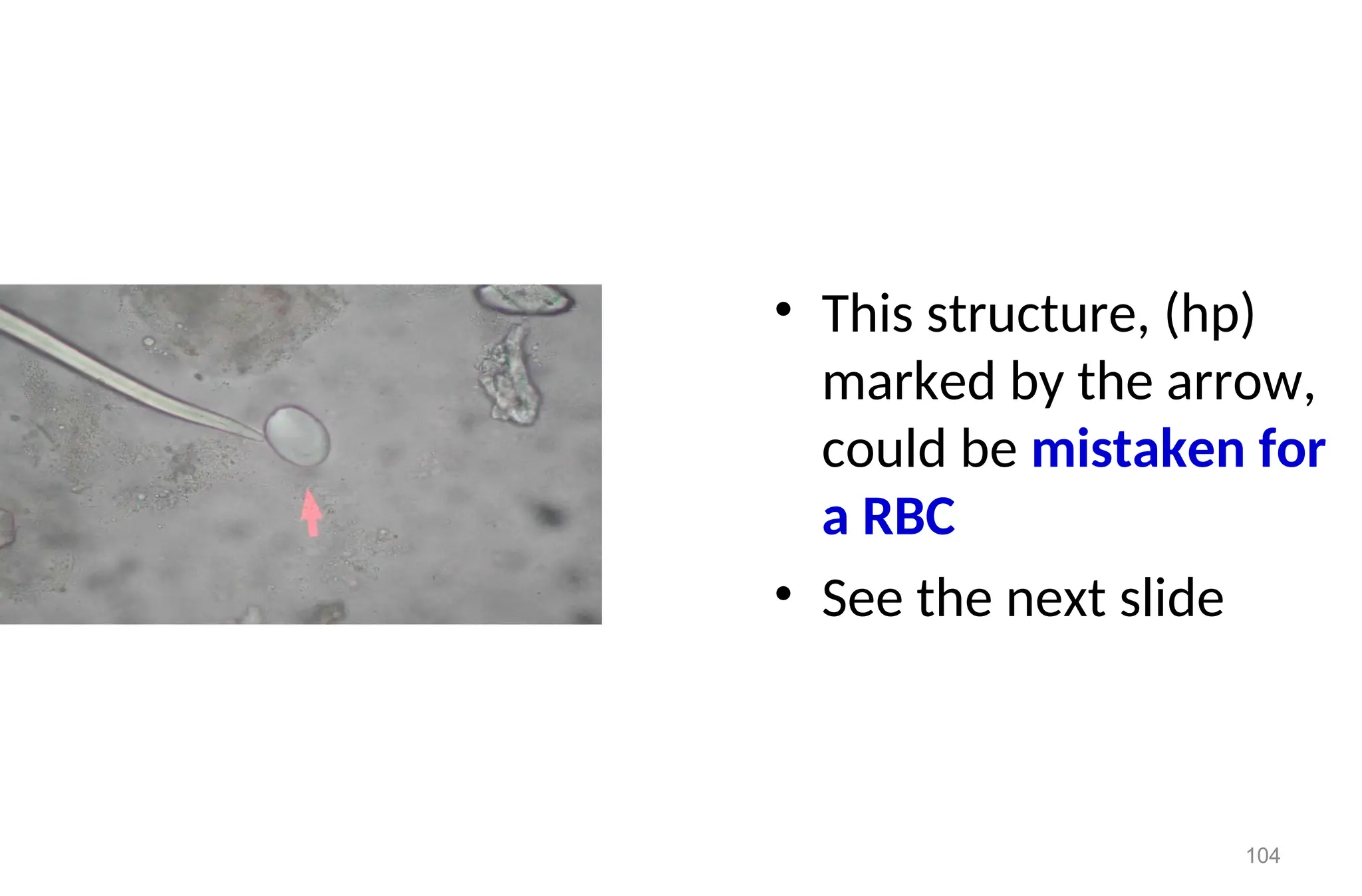
• This structure,(hp)
marked by the arrow,
could be mistaken for
a RBC
• See the next slide
105.
105
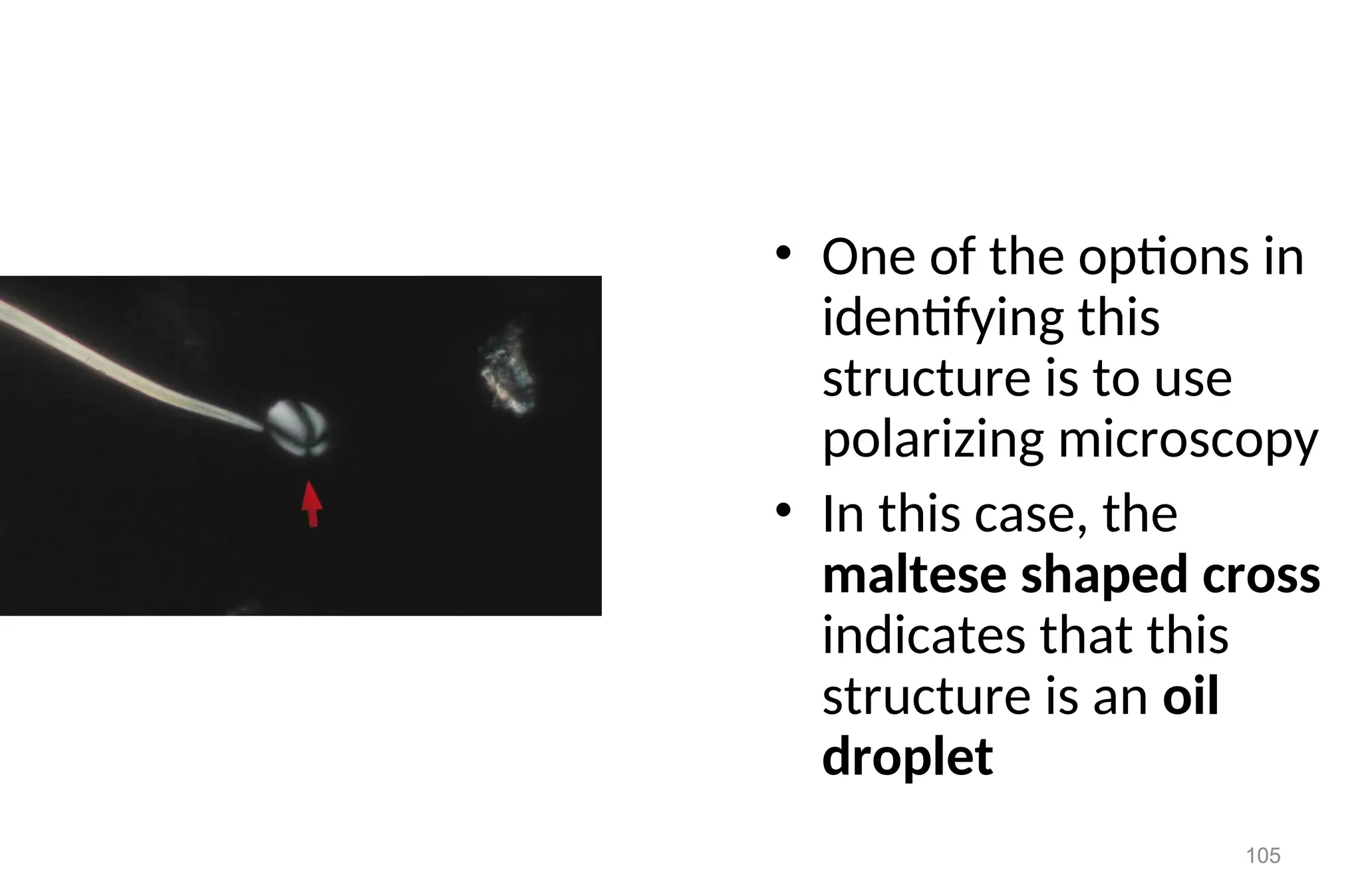
• One ofthe options in
identifying this
structure is to use
polarizing microscopy
• In this case, the
maltese shaped cross
indicates that this
structure is an oil
droplet
106.
106
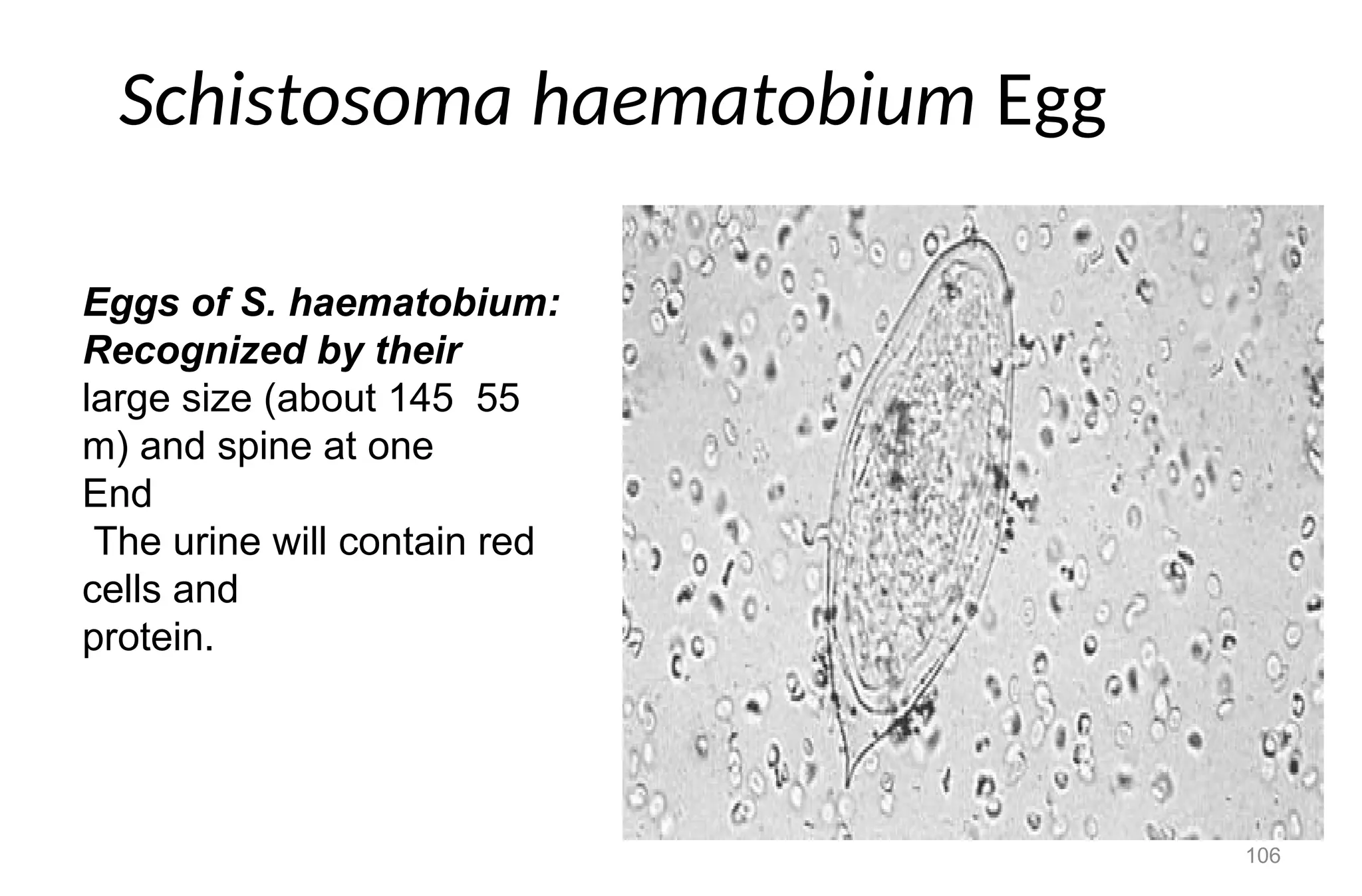
Schistosoma haematobium Egg
Eggsof S. haematobium:
Recognized by their
large size (about 145 55
m) and spine at one
End
The urine will contain red
cells and
protein.
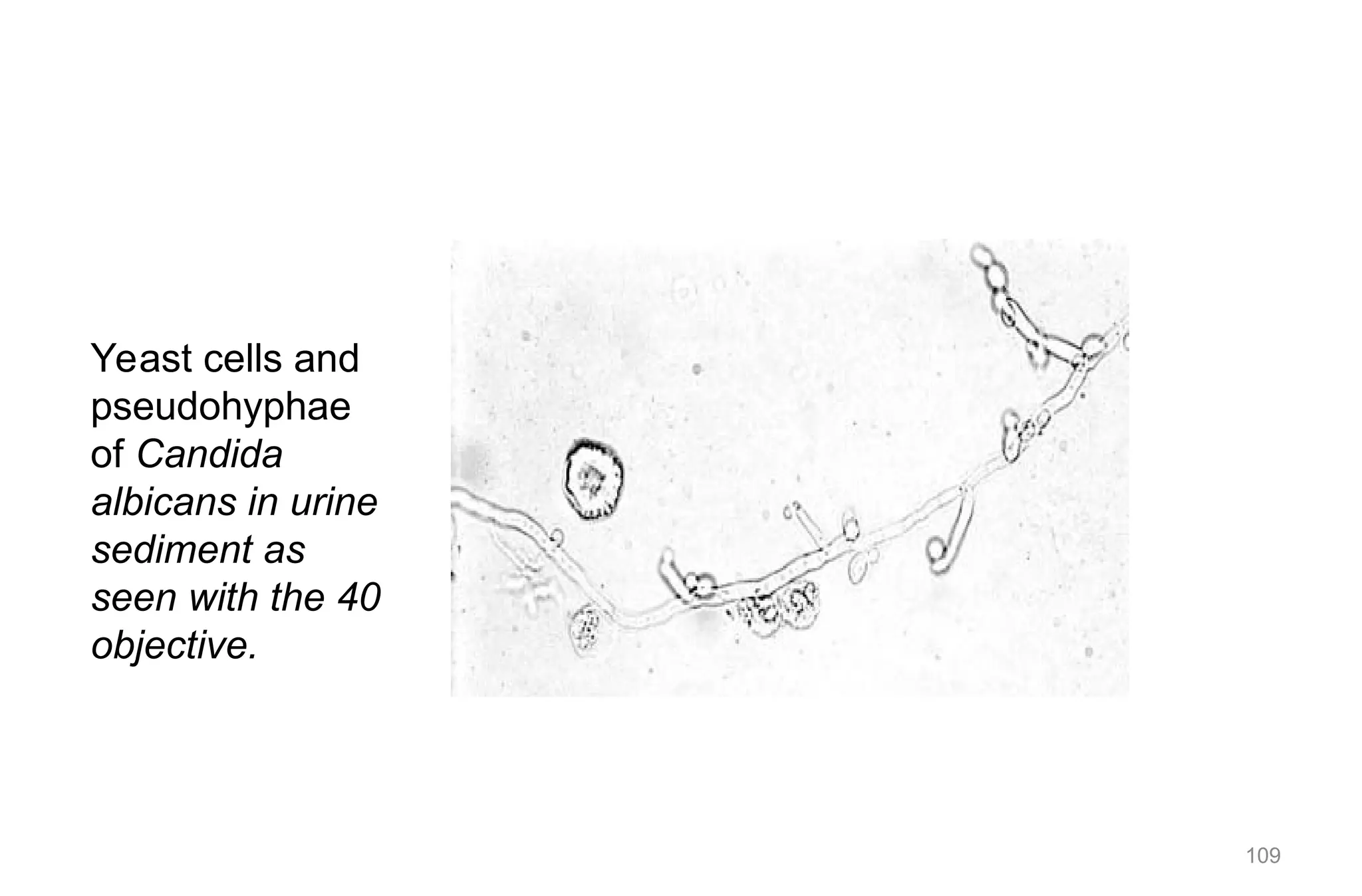
YEAST CELL
• Yeastcells are fungi that are not normally seen
in health individuals.
• Appearance
– Variable in size
– Colorless.
– Oval in shape, and usually form budding.
– Have high refractive index.
– Usually confused with Red Blood Cells.
108
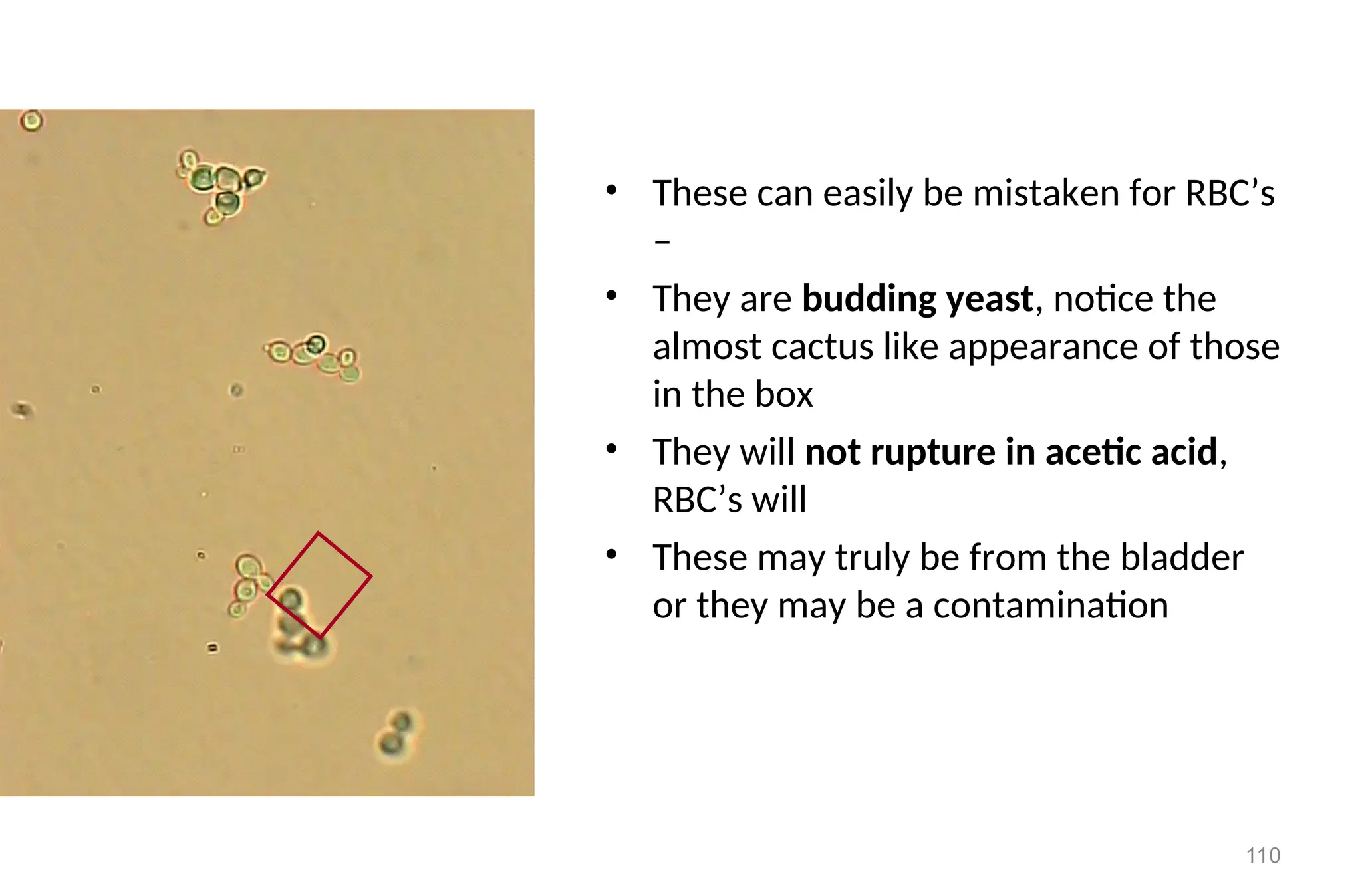
110
• These caneasily be mistaken for RBC’s
–
• They are budding yeast, notice the
almost cactus like appearance of those
in the box
• They will not rupture in acetic acid,
RBC’s will
• These may truly be from the bladder
or they may be a contamination
111.
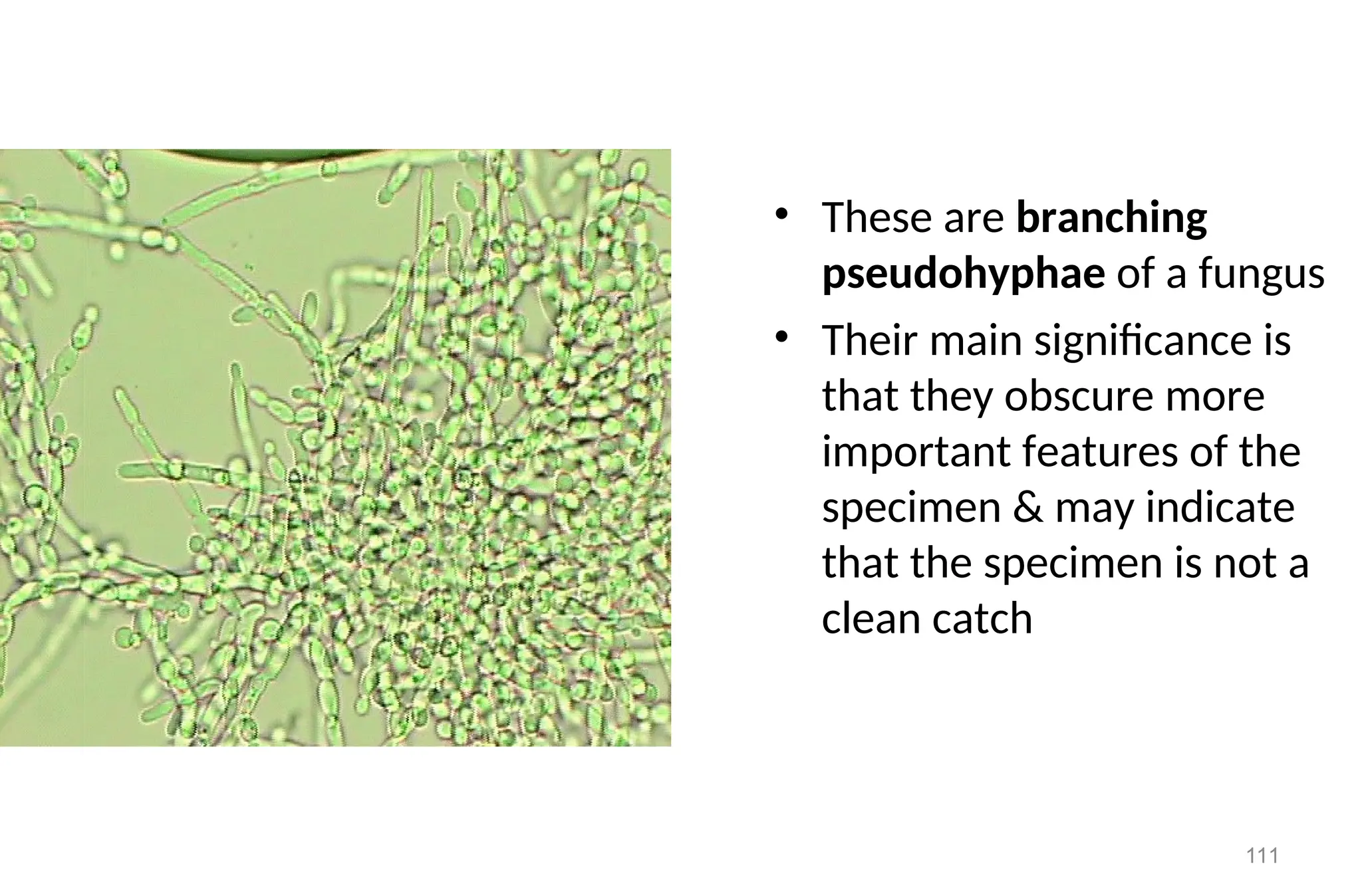
111
• These arebranching
pseudohyphae of a fungus
• Their main significance is
that they obscure more
important features of the
specimen & may indicate
that the specimen is not a
clean catch
112.
Clinical Significance
• Theyare usually of candida species (candida albicans) and are
common in patients with
– Urinary tract infection
– Vaginites
– Diabetic mellitus
– Intensive antibiotic or immunosuppressive therapy
112
113.
BACTERIA
• Bacteria arecommonly found in urine specimen because of
abundant normal microbial flora of the vagina or external urinary
meatus.
• Most common cause of UTI dipstick test can give indirect clue.
• Further the observed bacterial cell can be identified by
bacteriological culture
113
114.
BACTERIA cont”d
• Usuallyonly a single type of organism is present in
uncomplicated acute urinary infections.
• More than one type of organism is often seen in chronic and
recurring infections.
• Vaginal contamination of the specimen is indicated by a mixed
• bacterial flora (including Gram positive rods) and often the
presence of epithelial cells.
114
115.
Clinical Significance
• Presenceof bacteria may indicate the presence of UTI or
contamination by genital or intestinal microflora.
• Report of the Result
– Few bacteria / HPF
– Moderate bacteria / HPF
– Many bacteria / HPF
– Full of bacteria / HPF
115
116.
• Neisseria gonorrhoeaein urine
– In male patients with acute urethritis, it is often possible to
make a presumptive diagnosis of gonorrhoea by finding Gram
negative intracellular diplococci in pus cells passed in urine
116
118
Crystals in Sediment
•Crystals
– precipitation of solutes
– are not normally present in freshly voided urine
– can precipitate on storage
– most are not clinically significant
– pH critical to differentiating some important crystals
119.
119
Contributing factors to
CrystalFormation
• Concentration of solute in specimen
• Decreased flow of urine through tubules
• This enhances precipitation of solutes
• Ultrafiltrate can become supersaturated in tubules
120.
120
Crystals Correlate With:
•pH of urine
– solutes differ in solubility
– inorganic salts: oxalate, phosphate, calcium, ammonium
& magnesium less soluble in neutral or alkaline urine
– organic solutes: uric acid, bilirubin, & cystine less soluble
in acidic urine
121.
121
Acidic Urine
• Allclinically significant crystal are found in acid
urine
– Include: cystine, tyrosine, leucine & iatrogenic
crytsals: sulfonamide & ampicillin
122.
122
Acidic Urine
• AmorphousUrates
– Non crystalline urate salts of sodium, potassium,
magnesium & calcium
– small & yellow-brown granules - - similar to sand
– enhanced by refrigeration
– can be in acidic or neutral urine
123.
123
Amorphous Urates
• Willdissolve in alkaline or heated to 600
C
• If add acetic acid, uric acid crystals will precipitate
out
• Uroerythrin deposits on urate crystals giving pink-
organish color -- referred to as “brick dust”
124.
124
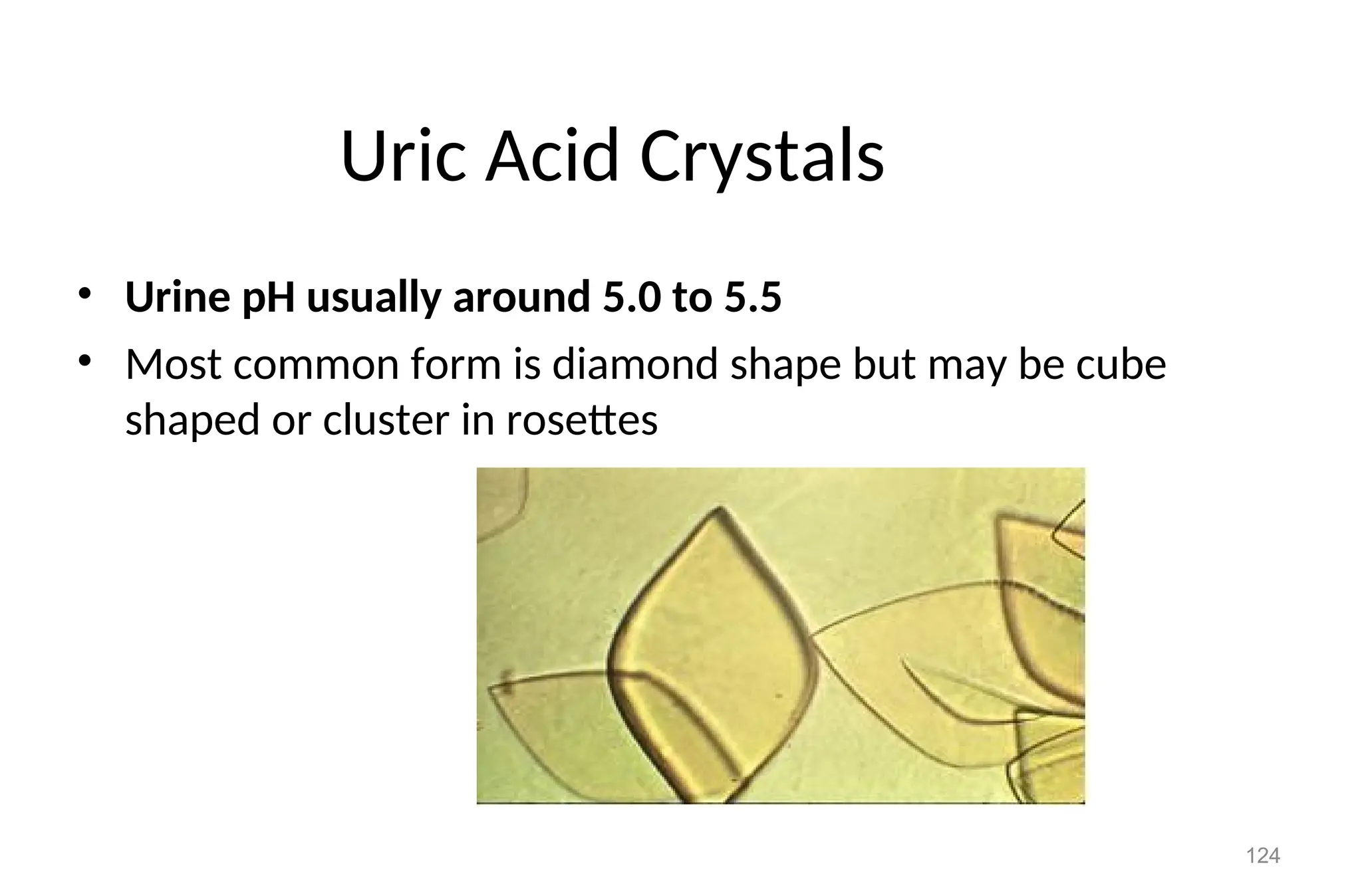
Uric Acid Crystals
•Urine pH usually around 5.0 to 5.5
• Most common form is diamond shape but may be cube
shaped or cluster in rosettes
125.
125
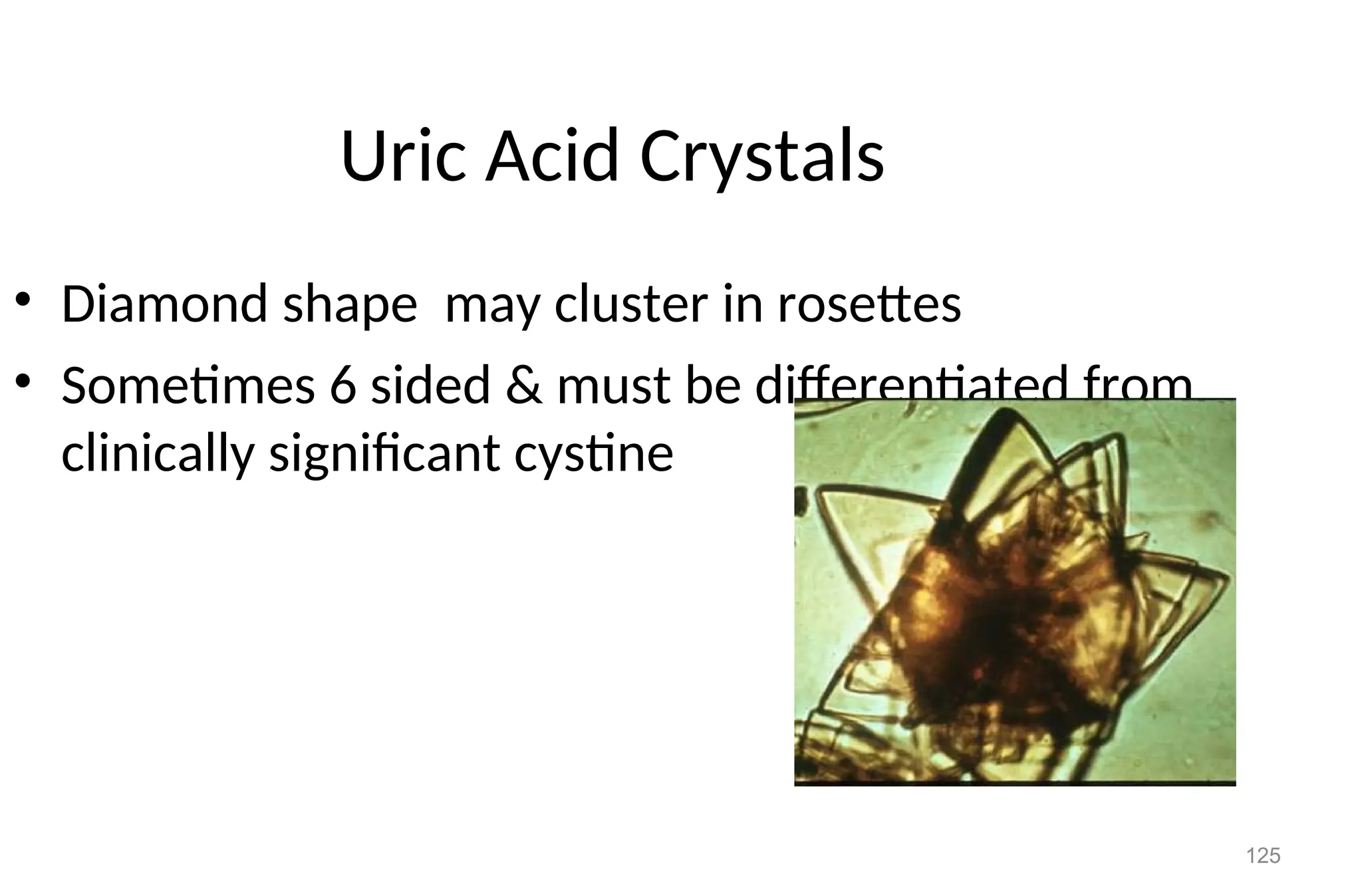
Uric Acid Crystals
•Diamond shape may cluster in rosettes
• Sometimes 6 sided & must be differentiated from
clinically significant cystine
126.
126
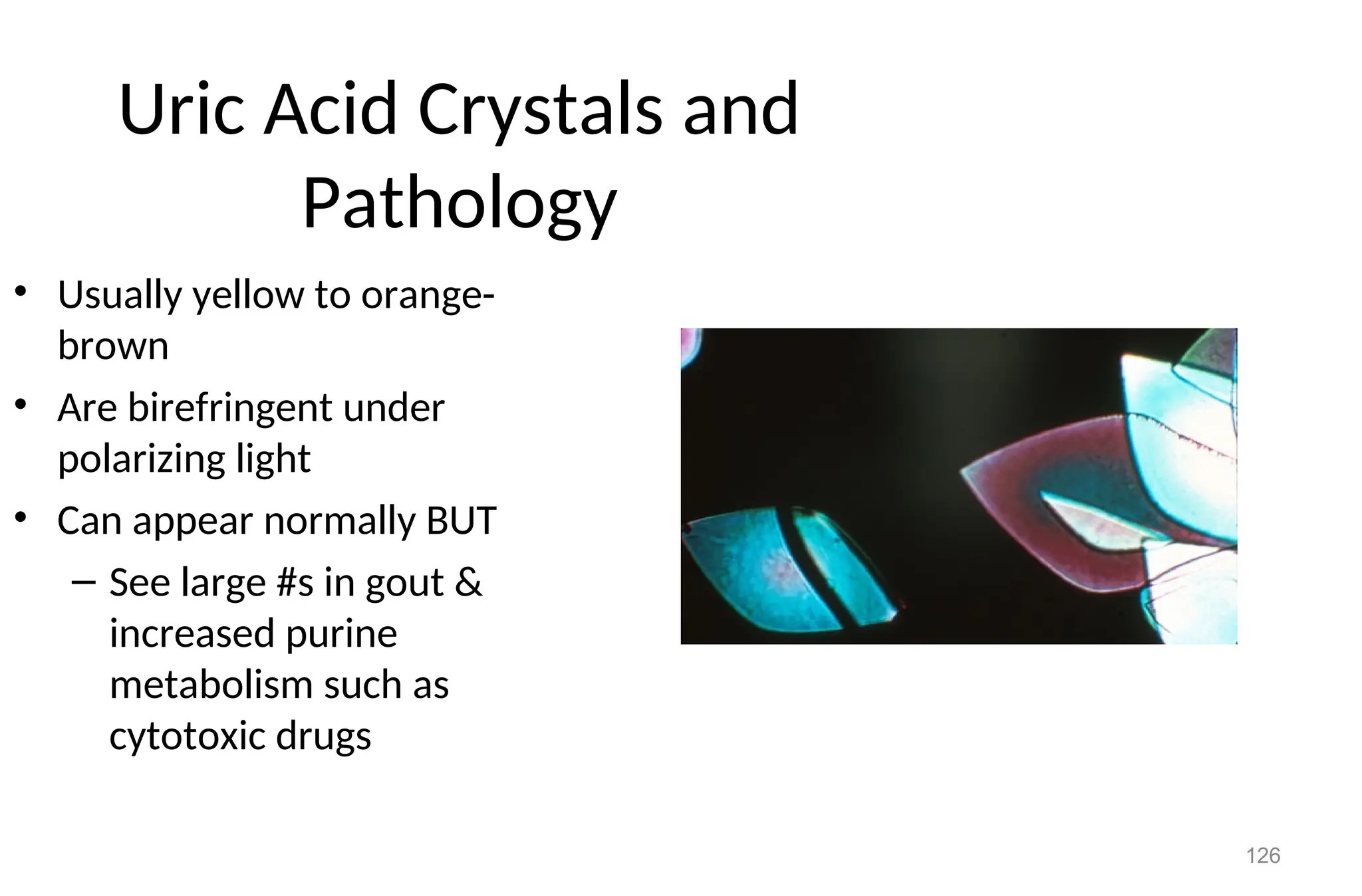
Uric Acid Crystalsand
Pathology
• Usually yellow to orange-
brown
• Are birefringent under
polarizing light
• Can appear normally BUT
– See large #s in gout &
increased purine
metabolism such as
cytotoxic drugs
127.
127
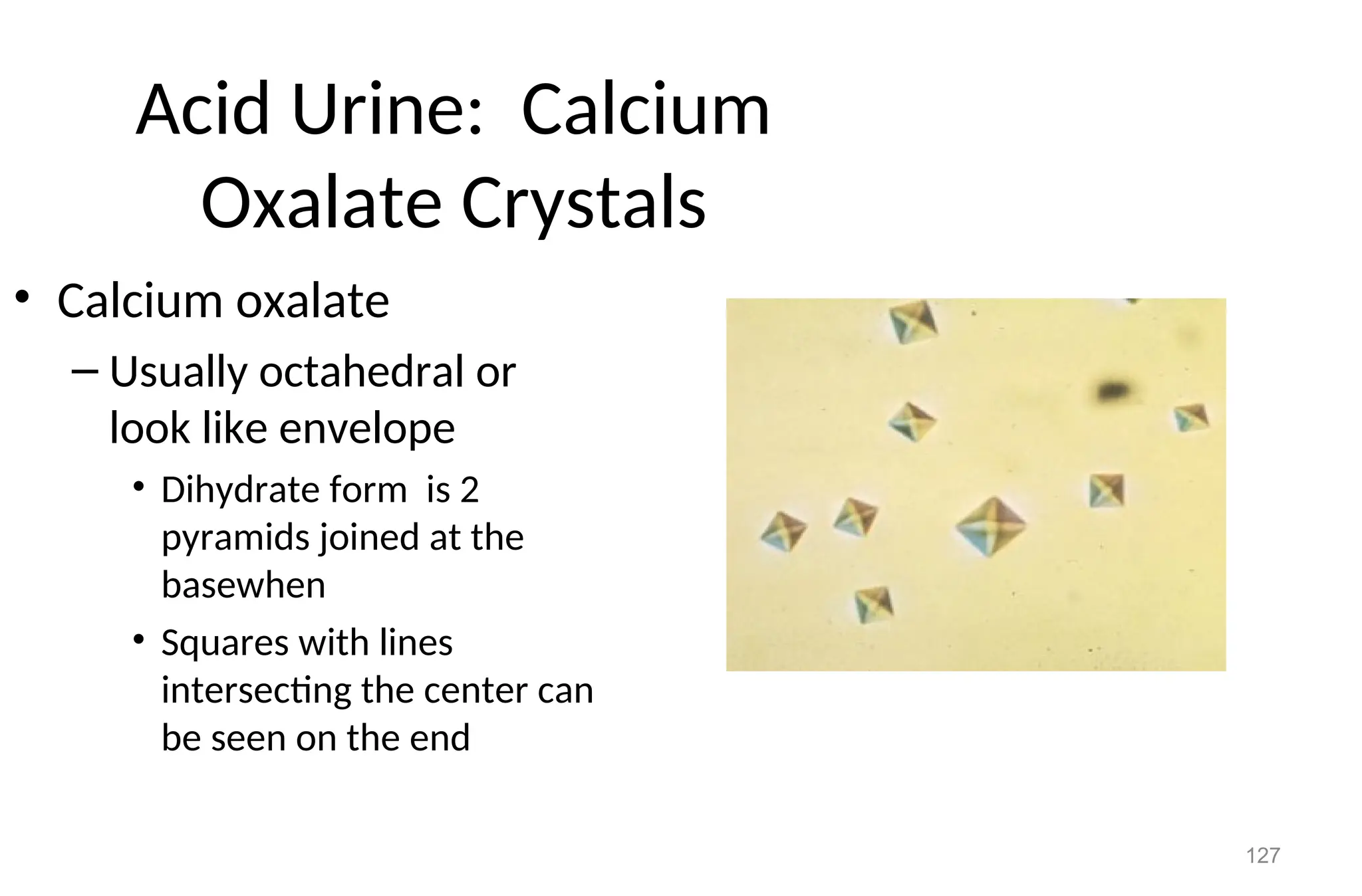
Acid Urine: Calcium
OxalateCrystals
• Calcium oxalate
– Usually octahedral or
look like envelope
• Dihydrate form is 2
pyramids joined at the
basewhen
• Squares with lines
intersecting the center can
be seen on the end
128.
128
Calcium Oxalate Crystals
•Monohydrate form - small ovoid or dumb bell
– rare & can mistake for RBC’s
– are birefringent under polarizing light
– are colorless & vary in size - usually small and may be in
either neutral or acidic urines
• Monohydrate form - small ovoid or dumb bell
– often see in normal urine, 2nd
to ascorbic acid, ingesting
tomatoes, asparagus, spinach & oranges
129.
129
Bilirubin
• Appear asfine needles, granules, or plates
– urine is acidic
– always yellow-brown
– the bile stains the other components of the
sediment
– presence of the crystals indicate high
concentrations of bilirubin in the urine
130.
130
Bilirubin Crystals: AbnormalState
• If you suspect bilirubin crystals are present, the strip
reaction must confirm the presence of bilirubin
• Otherwise the identification is incorrect
• The presence of the positive bilirubin strip &/or the
crystals indicate a pathologic process - are always
considered an abnormal crystal
• May see in liver disease
131.
131
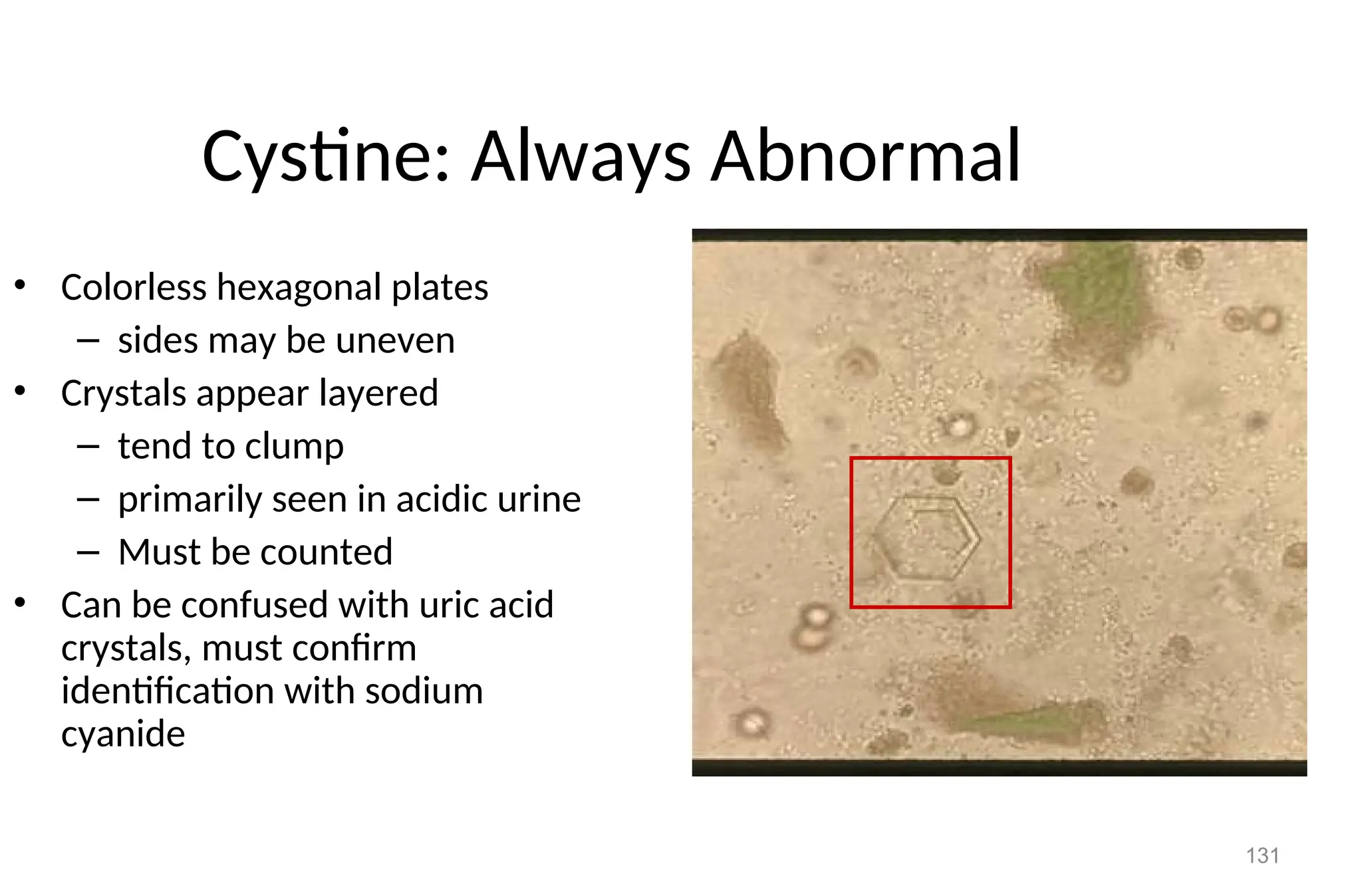
Cystine: Always Abnormal
•Colorless hexagonal plates
– sides may be uneven
• Crystals appear layered
– tend to clump
– primarily seen in acidic urine
– Must be counted
• Can be confused with uric acid
crystals, must confirm
identification with sodium
cyanide
132.
132
Cystine: Always Abnormal
•Clincally significant, seen in congenital cystinosis
or cystinuria
– Deposit out in tubules as calculi/stone causing
damage
133.
133
Amino Acid Crystals
•Tyrosine
– fine, delicate needles,
colorless or yellow
– frequently in clusters or
sheaves [as in stacks of
wheat]
– see singly or in small groups
– in acidic urine
– less soluble than leucine, so
found more often
134.
134
Leucine
• Highly refractileyellow to brown
spheres in acid urine.
• Have concentric/radial striations
on their surface
• Can be mistaken for fat globules
[or vice versa]
• But will not stain with fat stains or
appear as maltese cross under
polarization
• Can be seen in urine containing
tyrosine crystals if use alcohol to
‘precipitate’
Bactrim has similar appearance
check patient history
135.
135
Amino Acid Crystalsand
Pathology
• Amino acid crystals are abnormal & seen in
overflow aminoaciduria
– can be seen in rare cases of liver disease, more
likely to reflect inherited metabolic disorder
– before reporting should be confirmed by
confirmatory tests such as chromatography
136.
136
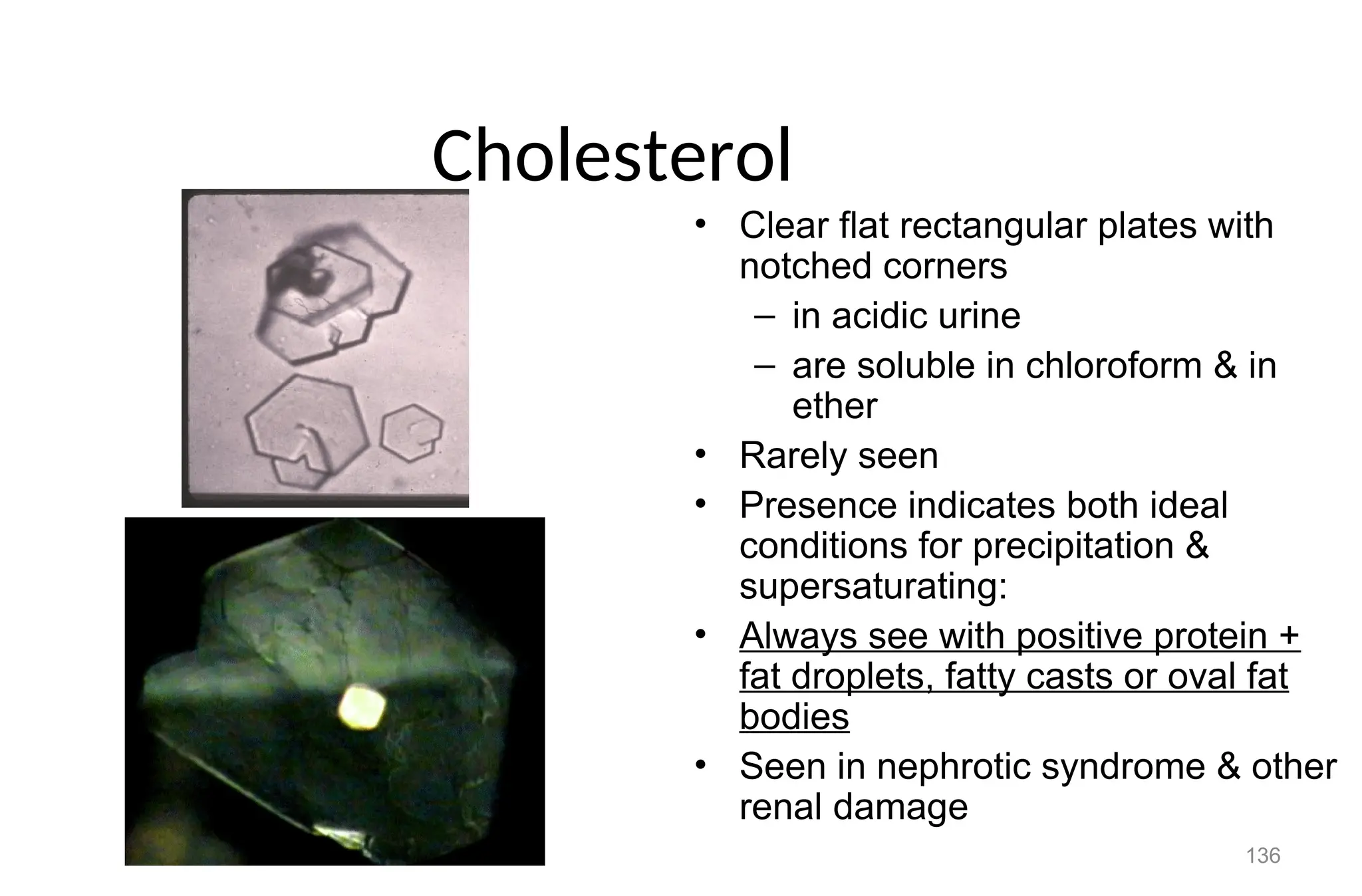
Cholesterol
• Clear flatrectangular plates with
notched corners
– in acidic urine
– are soluble in chloroform & in
ether
• Rarely seen
• Presence indicates both ideal
conditions for precipitation &
supersaturating:
• Always see with positive protein +
fat droplets, fatty casts or oval fat
bodies
• Seen in nephrotic syndrome & other
renal damage
137.
137
Confounding Conditions
• Diatrizoatemeglumine [radiopaque contrast medium] can be
mistaken for cholesterol
– contrast medium will give abnormally high S.G. >1.040
– not associated with proteinuria or lipiduria
– cholesterol crystals found with normal S.G.
• Medications
– can be excreted in high concentrations, resulting in precipitation
– these crystals are termed ‘iatrogenic’
– proper identification of drug crystals important in alerting to
potential renal tubular damage
138.
138
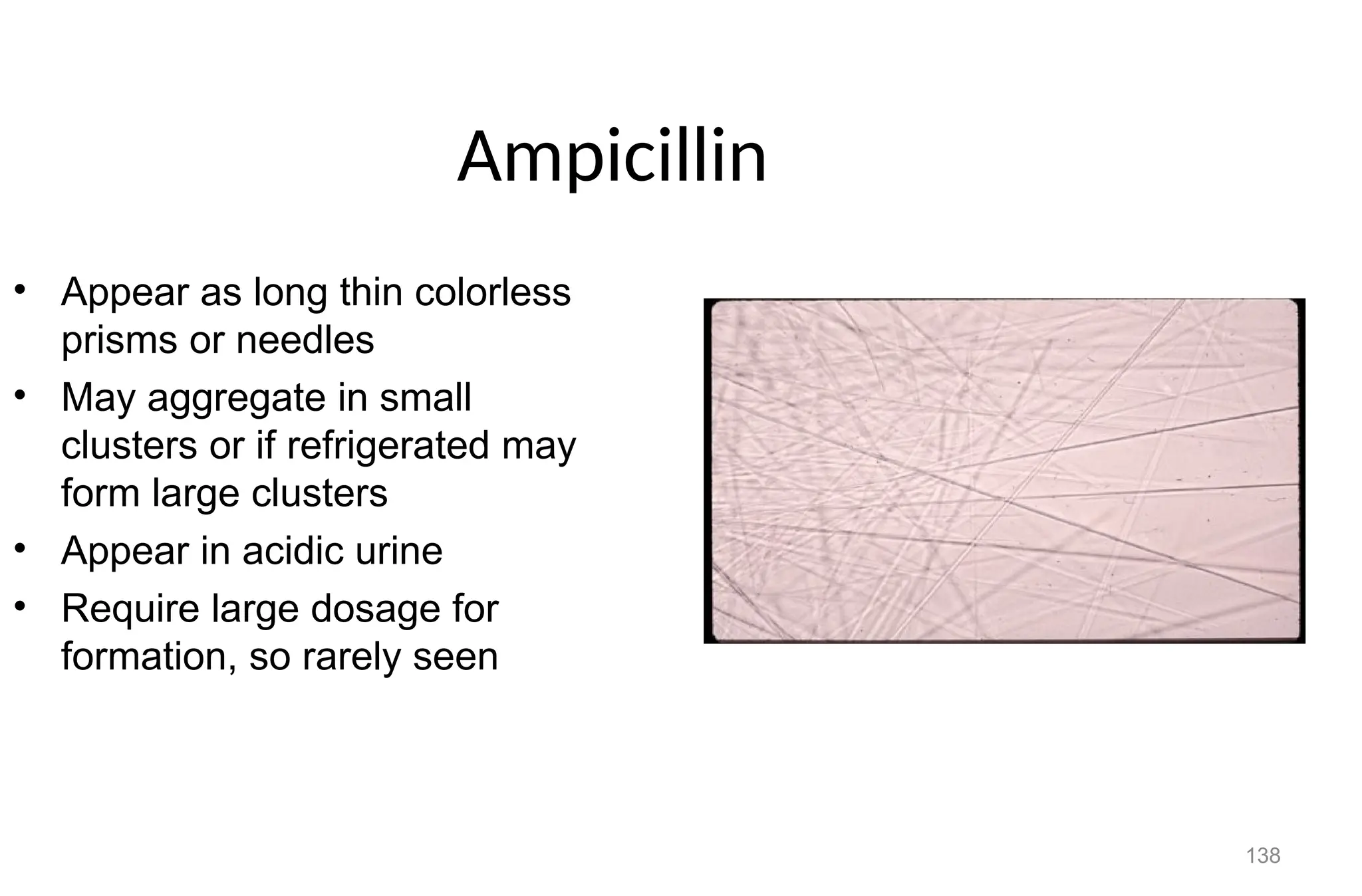
Ampicillin
• Appear aslong thin colorless
prisms or needles
• May aggregate in small
clusters or if refrigerated may
form large clusters
• Appear in acidic urine
• Require large dosage for
formation, so rarely seen
139.
139
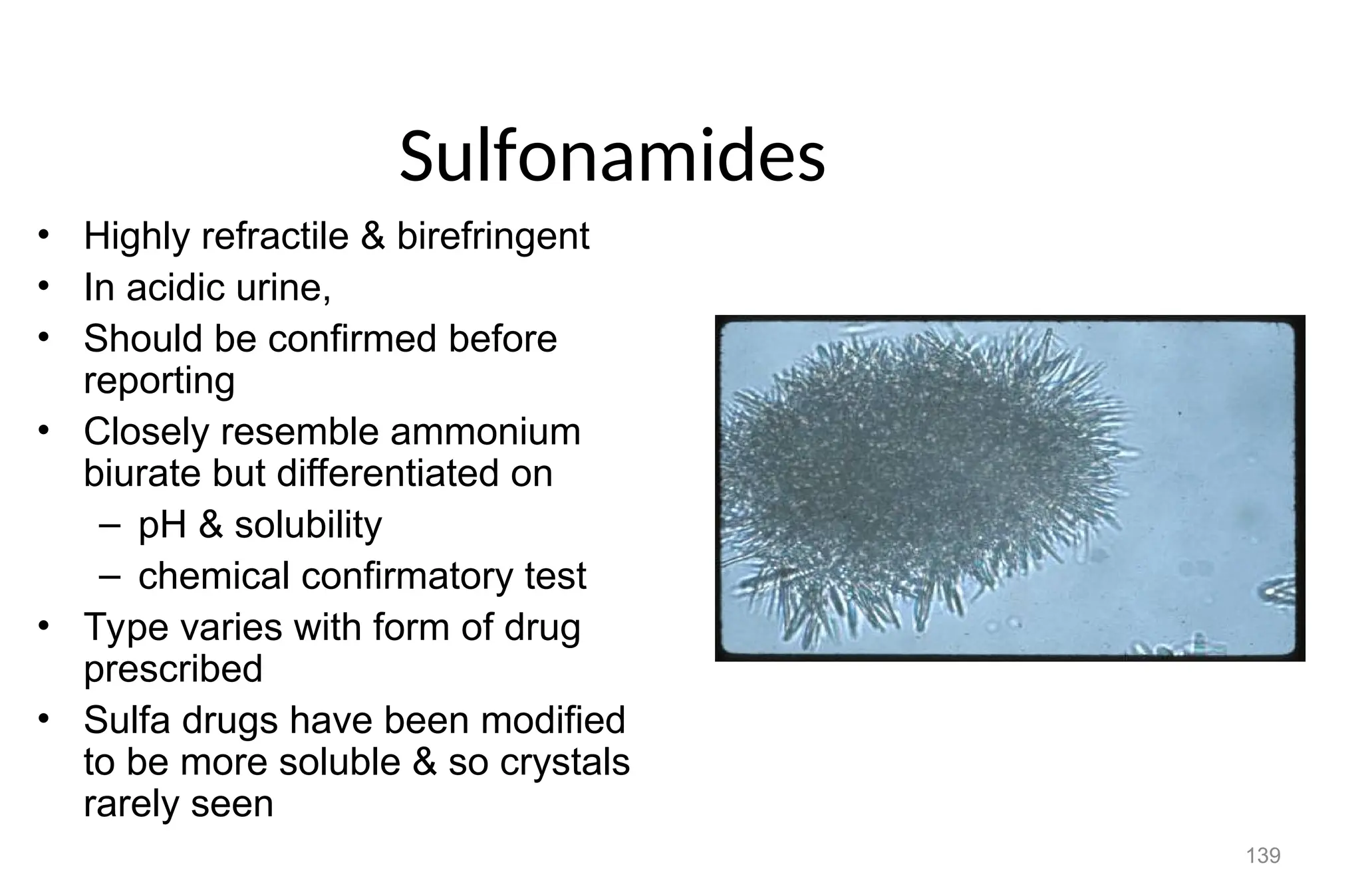
Sulfonamides
• Highly refractile& birefringent
• In acidic urine,
• Should be confirmed before
reporting
• Closely resemble ammonium
biurate but differentiated on
– pH & solubility
– chemical confirmatory test
• Type varies with form of drug
prescribed
• Sulfa drugs have been modified
to be more soluble & so crystals
rarely seen
140.
140
• Sulfadiazine crystalsappear
yellow to brown & as bundles of
wheat
– constriction may be central
or excentric
• Sulfamethoxazole [Bactrim &
Septra] more commonly seen
– brown rosettes or spheres
with irregular striations
141.
141
Radiographic Contrast Media
•Diatrizoate salts are used in IV contrast media
• Readily soluble in water & excreted in urine
• Diatrizoate meglumine [Renografin]
– crystals colorless, long pointed needles, singly or in clusters
or
– flat elongated rectangular plates
• distinguished from cholesterol by large # present & high
S.G. [>1.040]
• lack significant proteinuria & lipiduria
• diatrizoate appears in acidic urine up to 4 hrs post injection
– can cause false pos. sulfosalicylic acid test
142.
142
Alkaline Urine Crystals
•Ammonium Phosphate
– alkaline or neutral urine
– microscopically not distinguishable from amorphous urates
• distinguishable on urine pH & solubility
• precipitate white rather than pink-orange of amorphous
urates
• are soluble in acid & will not dissolve when heated to 60C
– fine colorless grains with tendency to obscure other more
significant sediment
– presence enhanced by refrigeration
143.
143
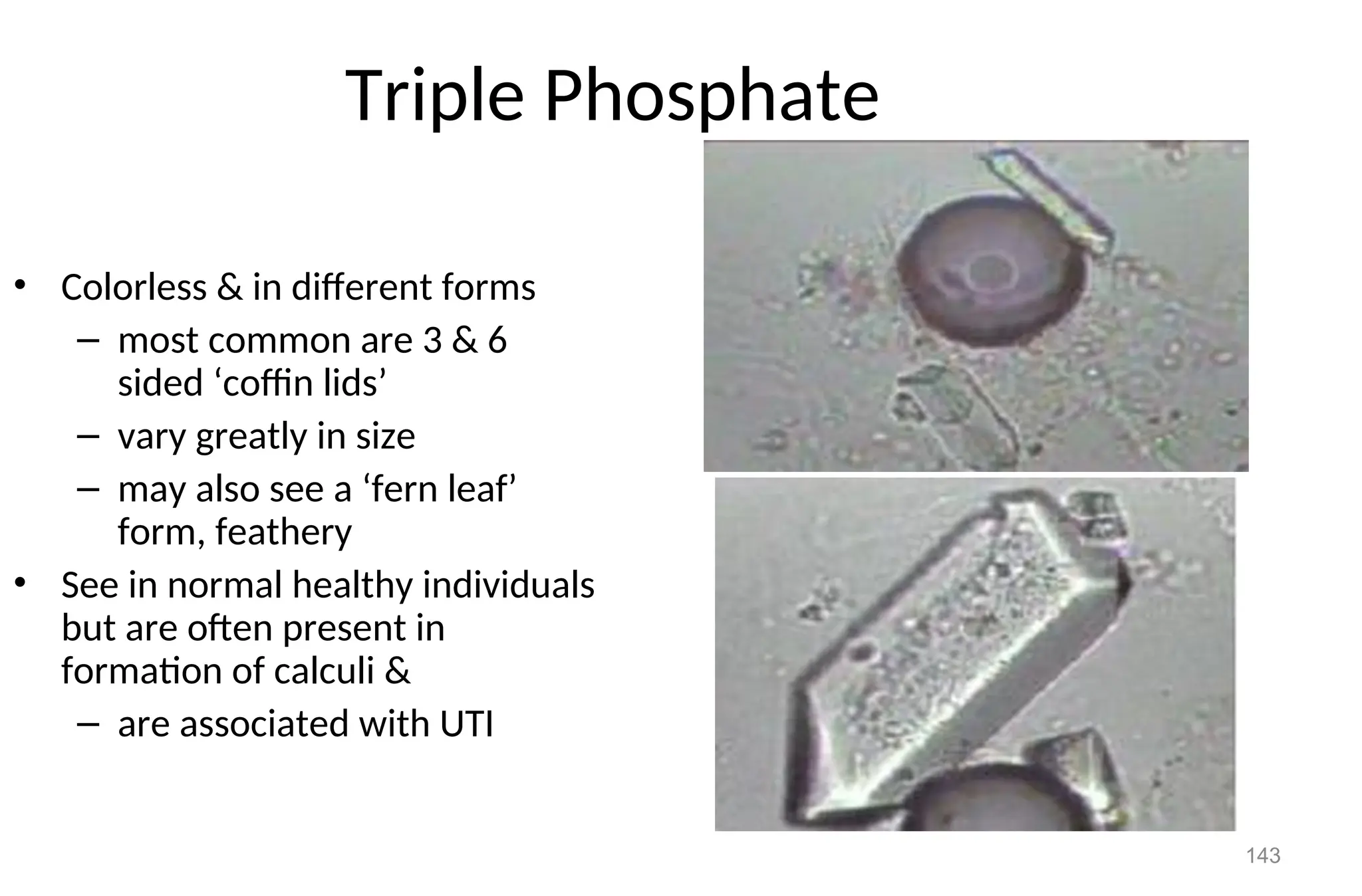
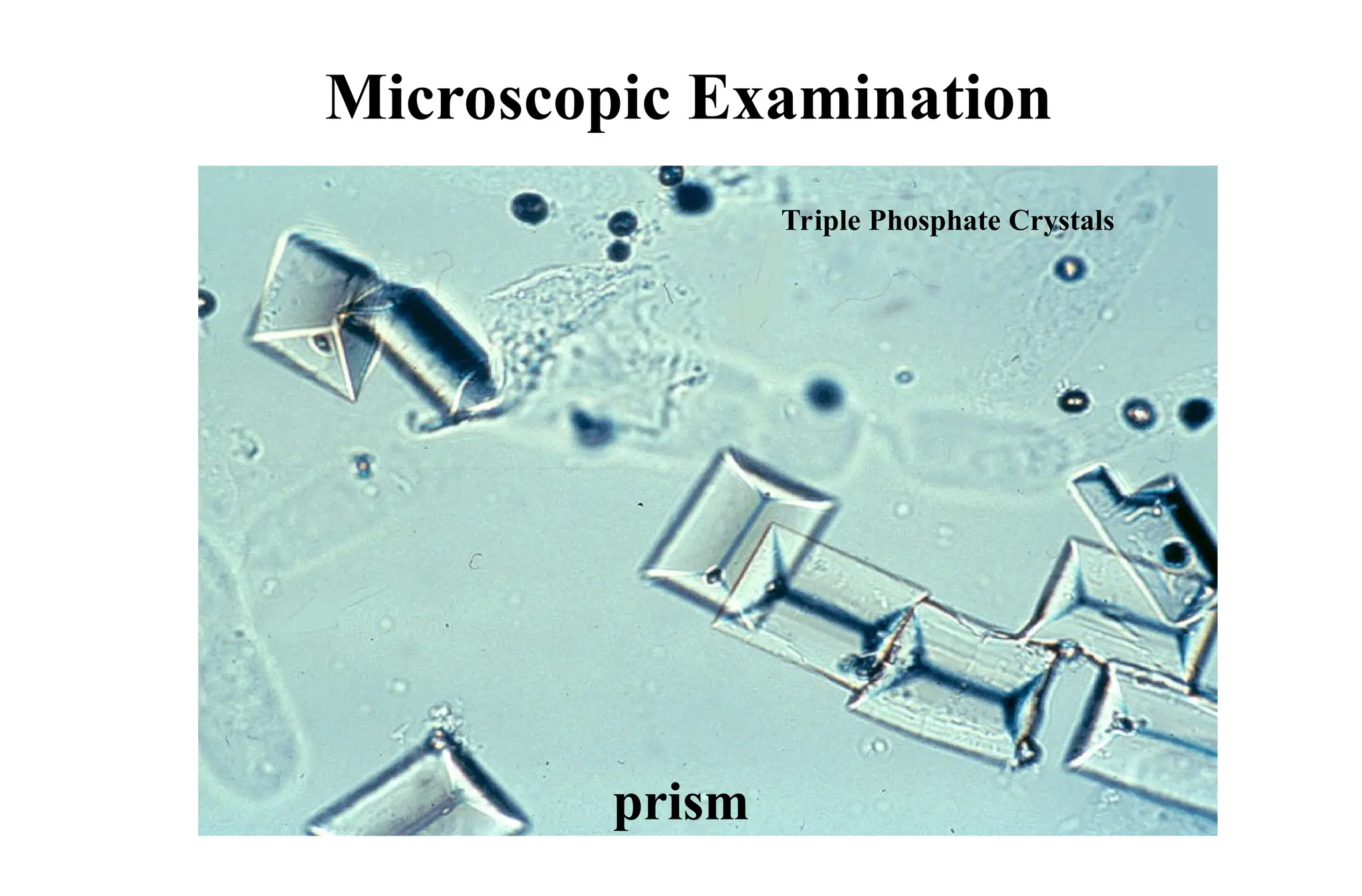
Triple Phosphate
• Colorless& in different forms
– most common are 3 & 6
sided ‘coffin lids’
– vary greatly in size
– may also see a ‘fern leaf’
form, feathery
• See in normal healthy individuals
but are often present in
formation of calculi &
– are associated with UTI
145
Calcium Phosphate
• In2 forms dicalcium & calcium
• Dicalcium colorless thin prisms in rosettes or star-
shaped ‘stellar phosphates’
– tend to have 1 tapered or pointed end & the other
squared off
– calcium phosphates are irregular granular sheets or plates
- - often resemble degenerating squamous epithelial cells
146.
146
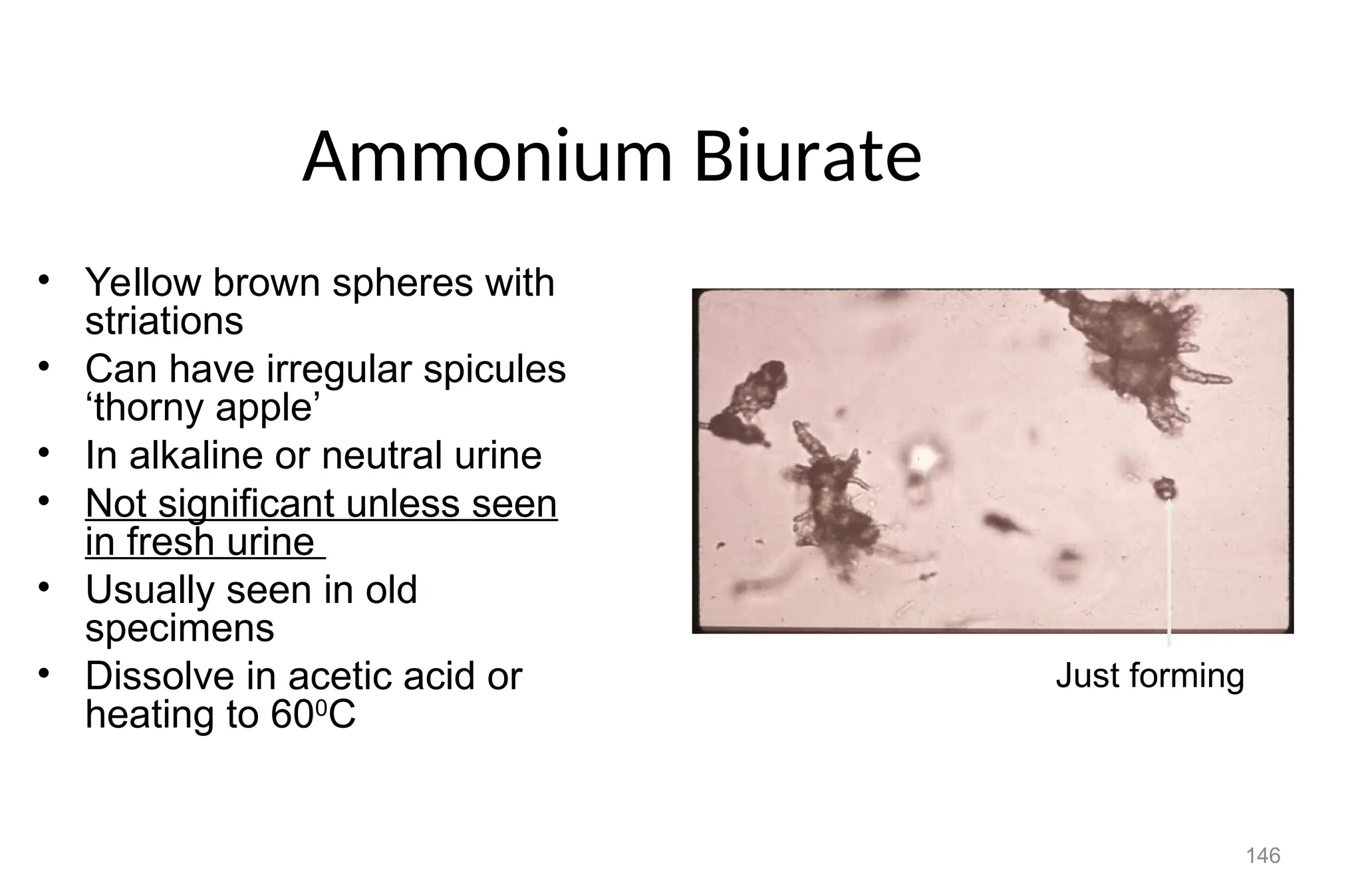
Ammonium Biurate
• Yellowbrown spheres with
striations
• Can have irregular spicules
‘thorny apple’
• In alkaline or neutral urine
• Not significant unless seen
in fresh urine
• Usually seen in old
specimens
• Dissolve in acetic acid or
heating to 600
C
Just forming
147.
147
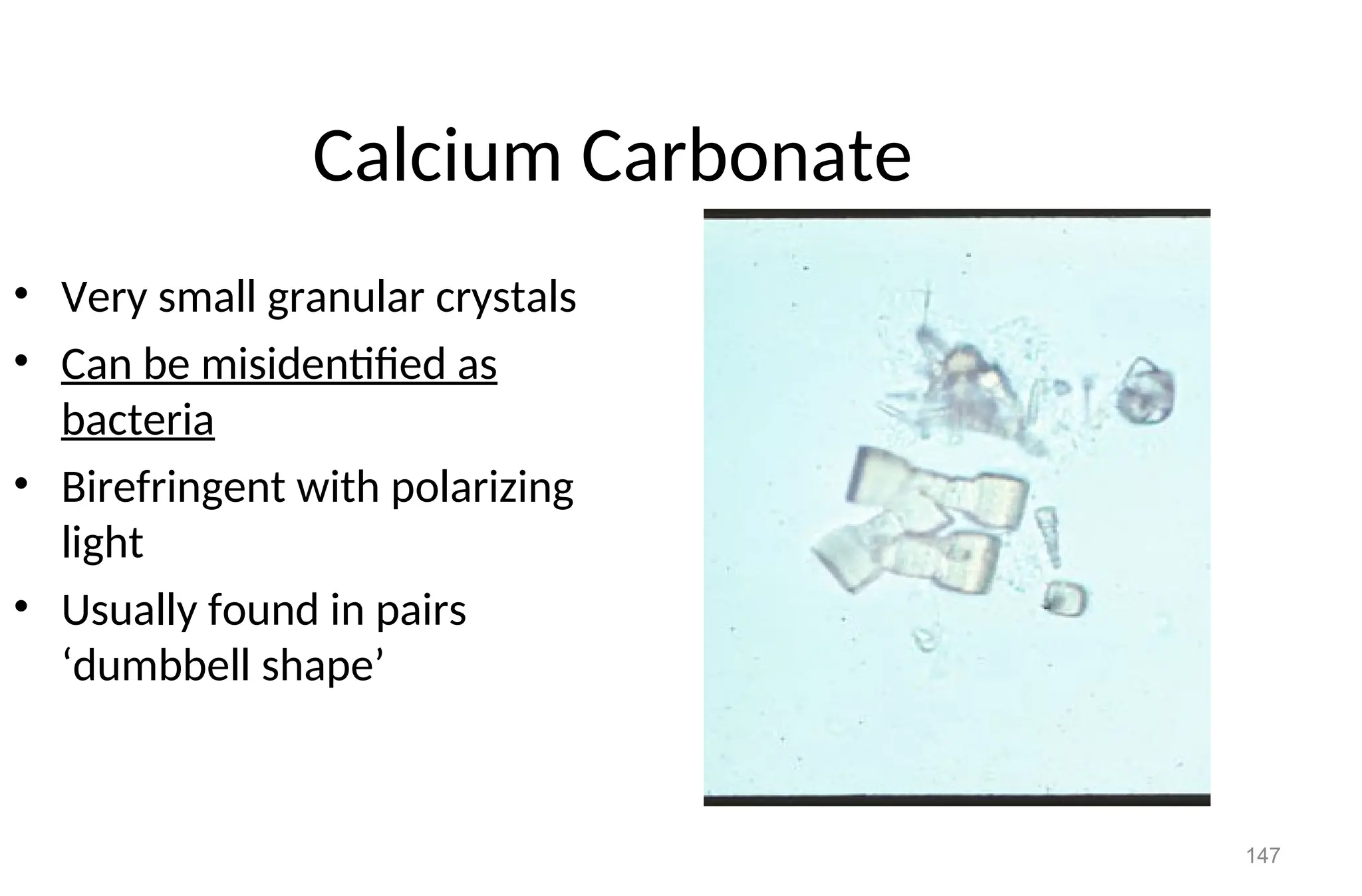
Calcium Carbonate
• Verysmall granular crystals
• Can be misidentified as
bacteria
• Birefringent with polarizing
light
• Usually found in pairs
‘dumbbell shape’
148.
Cystine Crystals
Rarelyfound.
Flat, hexagonal plates with well defined edges.
Colorless, and highly retractile.
Size is 30-60 m.
Found only in fresh urine, because if there is delay, they are
soluble and not seen.
Appeared during cystinosis, which is a hereditary disease
(Wilson disease), or during transient acute phase of
pyelonephritis. Its appearance in the urine is called cystinuria.
148
149.
Calcium Sulfate Crystals
Have large prism or flat bladder shaped.
Seen separately or in bundles.
Size 50-100 m.
Can be distinguished from calcium phosphate
crystals by measuring pH of urine.
149
150.
MISCELLANEOUS
Spermatozoa
• Are smallstructures consisting of a head and tail, connected by a
short middle piece (neck).
• Easily recognized especially if they are motile.
• Frequently seen in the urine of males.
• They may see in the urine of females, when the urine collected
after coitus usually not reported, unless the physician has special
interest in it.
150
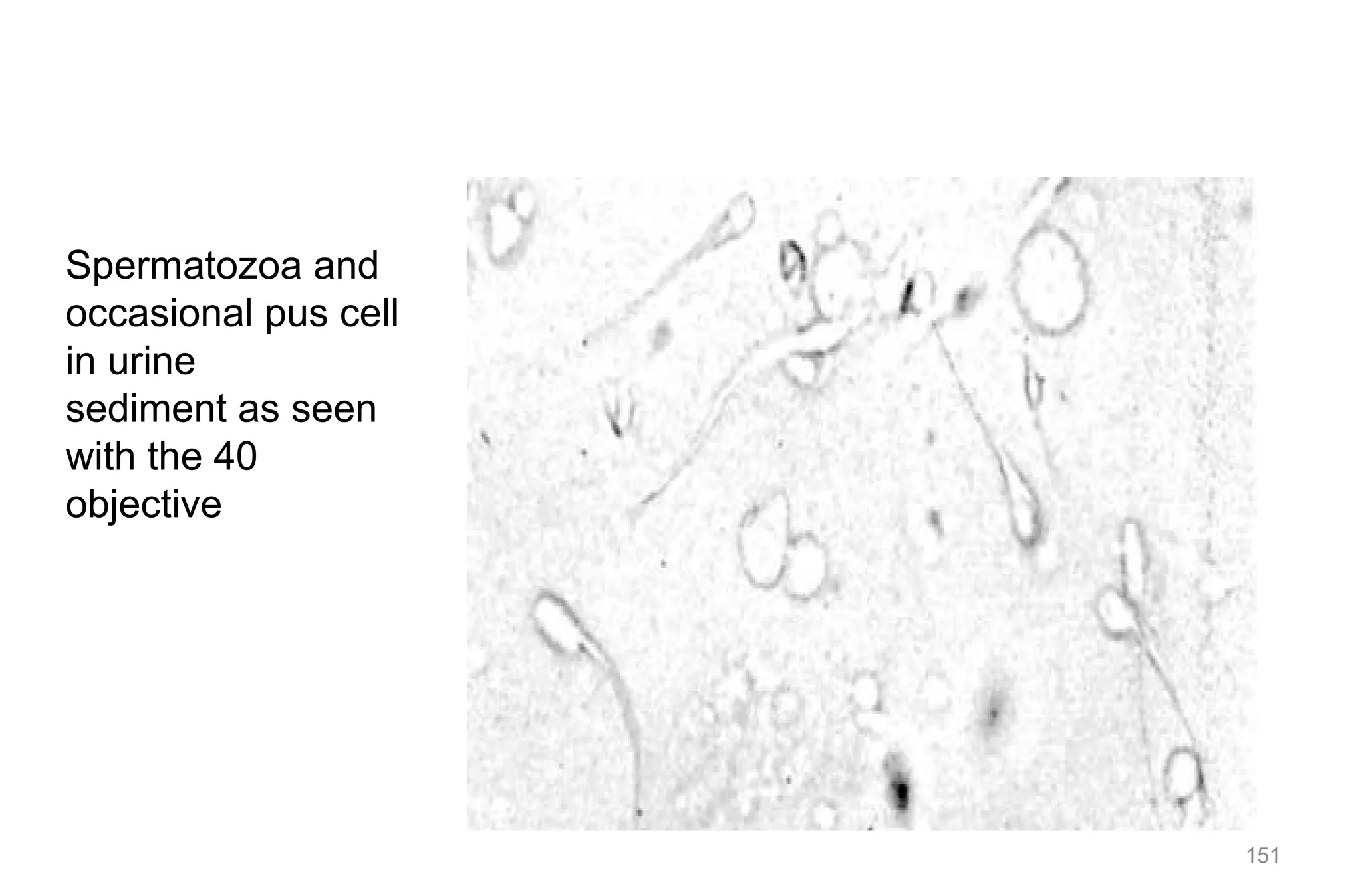
152
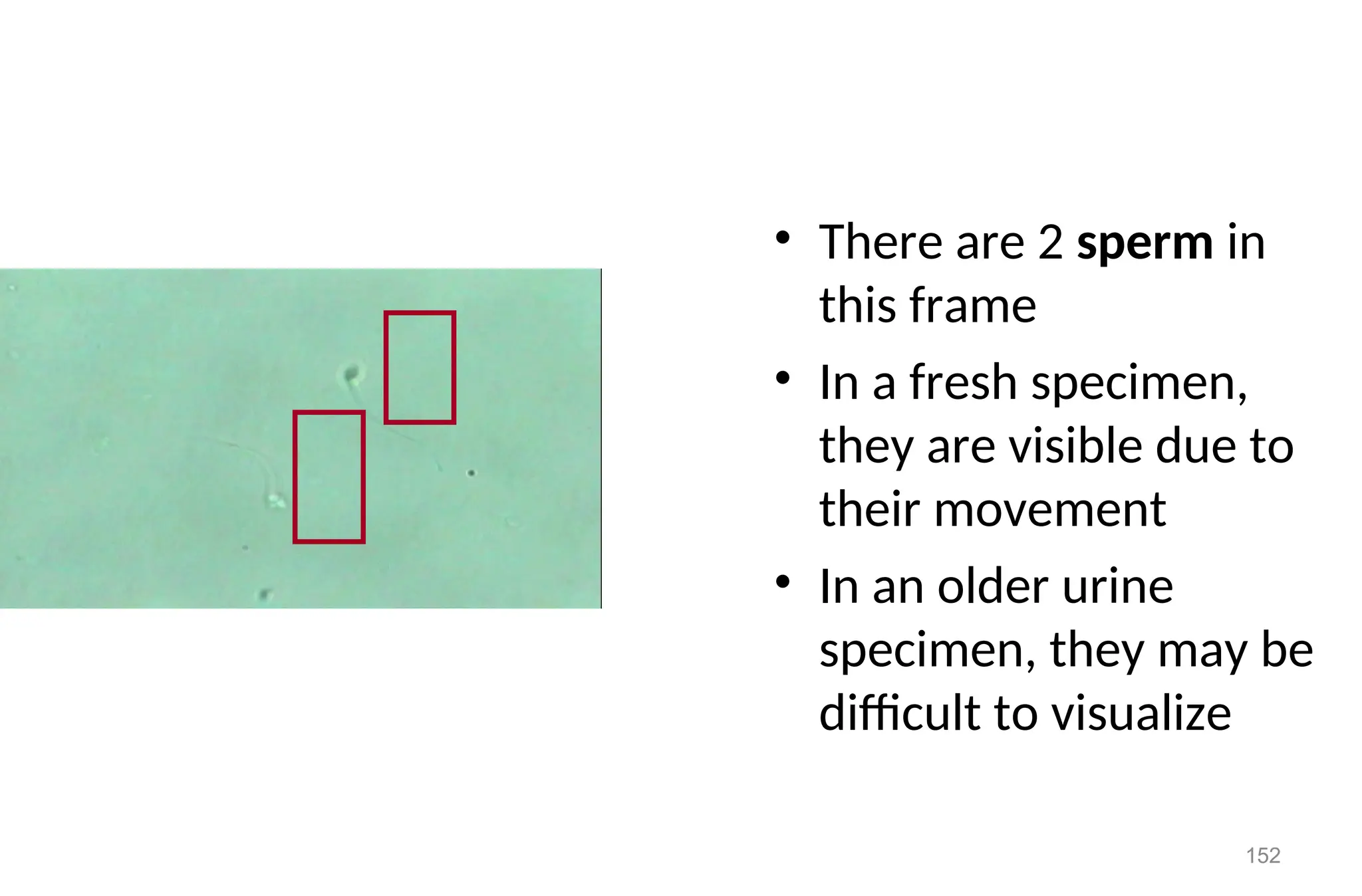
• There are2 sperm in
this frame
• In a fresh specimen,
they are visible due to
their movement
• In an older urine
specimen, they may be
difficult to visualize
153.
153
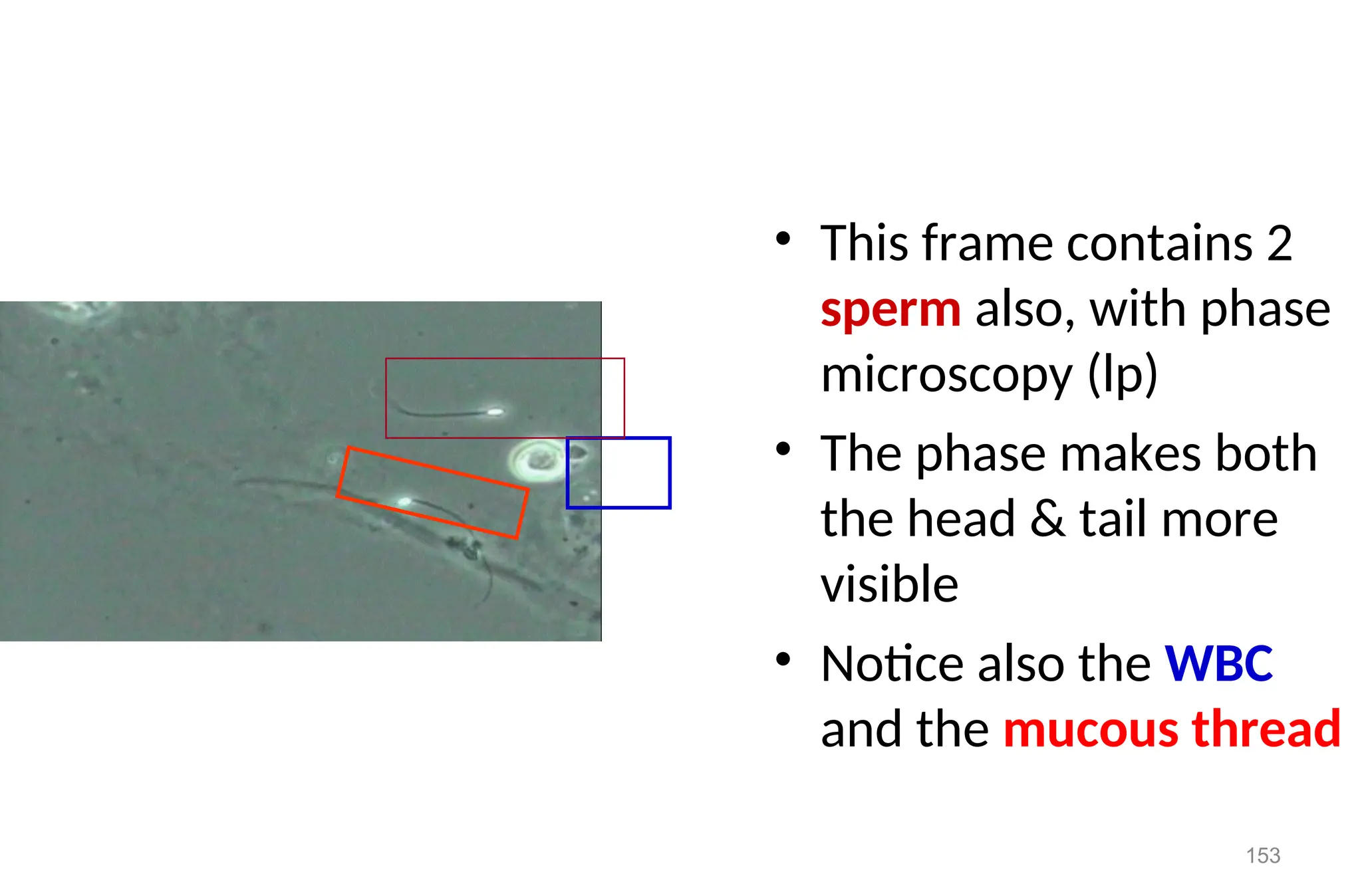
• This framecontains 2
sperm also, with phase
microscopy (lp)
• The phase makes both
the head & tail more
visible
• Notice also the WBC
and the mucous thread
154.
Mucus Trades
• Formedby the precipitation of mucoprotein in cooled urine.
• Have fine, fiber like appearance.
• Wavy in shape and tapered at ends.
• If not examined carefully may confuse with hyaline casts.
154
155.
Contaminates and ArtifactStructure
Muscle fibers
• Vegetable cells
• Structure from slide or cover slide
• Fat droplets (other bubbles)
• Oil droplets
• Pollen greens
• Starch granules
155
156.
156
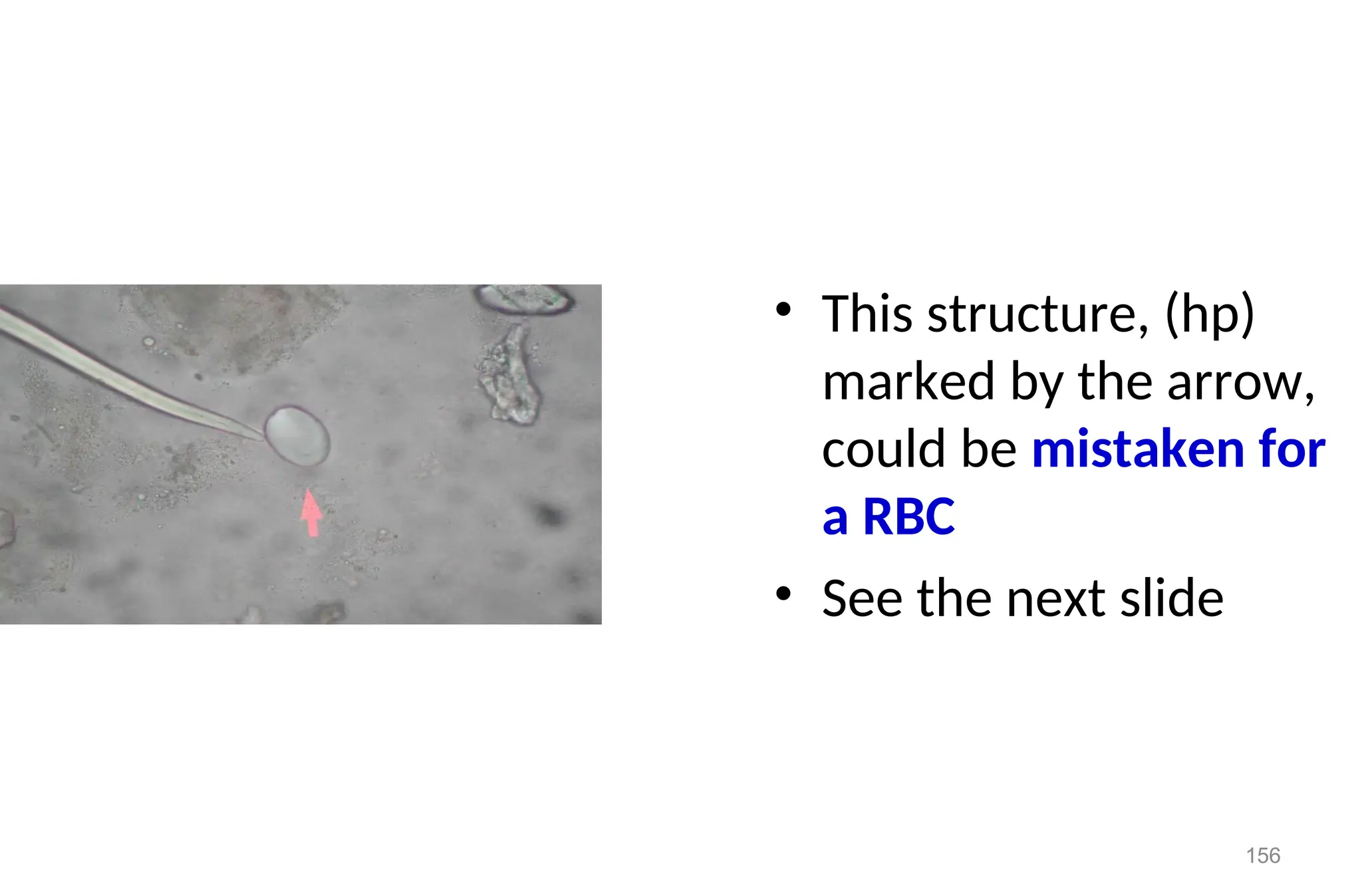
• This structure,(hp)
marked by the arrow,
could be mistaken for
a RBC
• See the next slide
157.
157
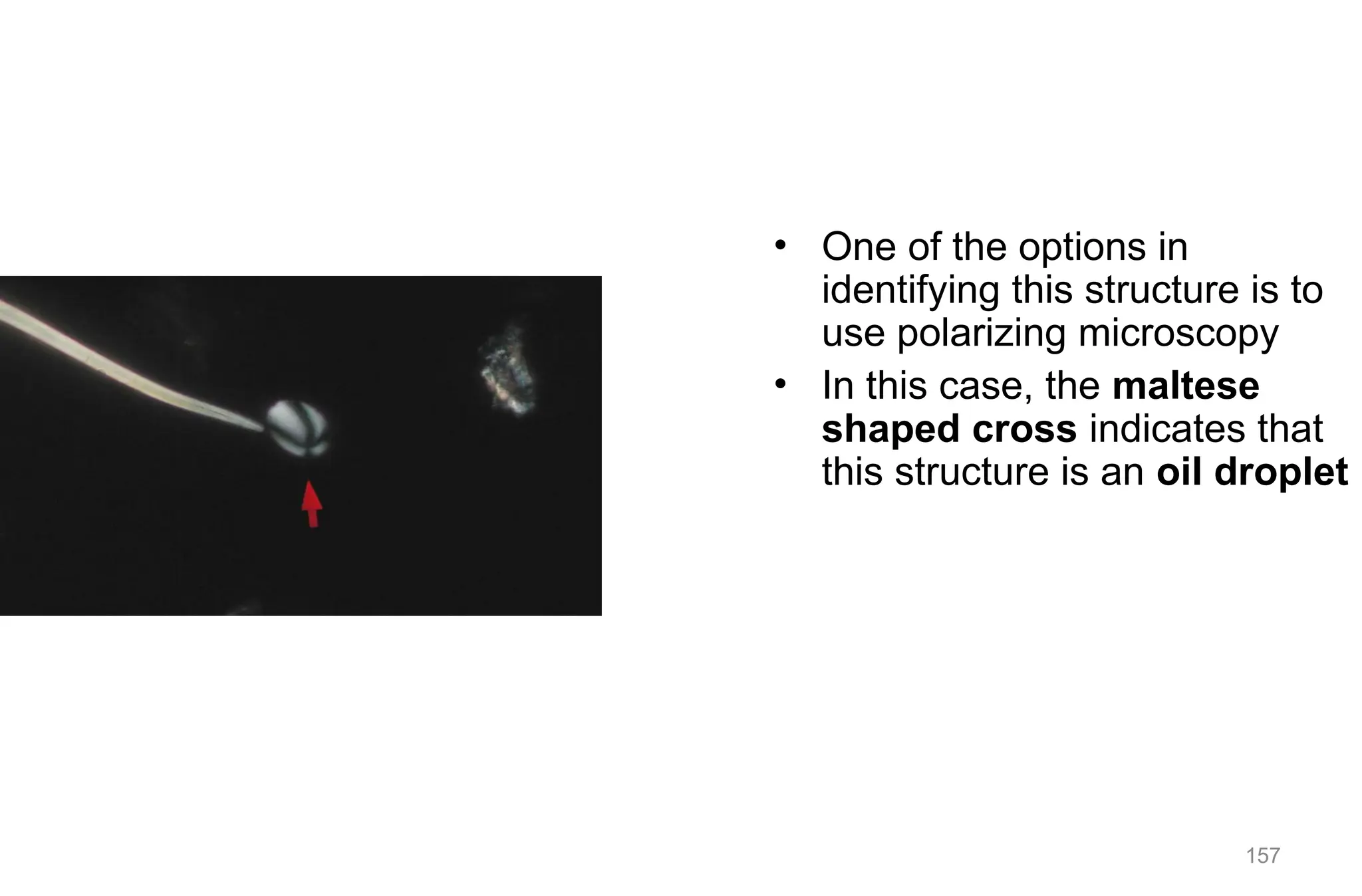
• One ofthe options in
identifying this structure is to
use polarizing microscopy
• In this case, the maltese
shaped cross indicates that
this structure is an oil droplet
158.
Methods for ExaminingUrine
Sediments
Unstained Urine Sediment and Stained Preparation
Unstained Urine Sediment Preparation
Bright field microscopy of the unstained urine sediment
Phase Contrasts (PC)
158
159.
Stained Preparation
(a) Acrystal violet safranin stain (sternheimer and malbin) is useful in the
identification of cellular elements. Staining reaction to crystal – violet safranin
stain:
RBC – Purple to dark purple.
WBC – Cytoplasm -violet to blue.
Nucleus – reddish purple.
Glitter cells – blue .
159
Automations in Urinalysis
•automations are utilized in urinalysis laboratories.
• These machines can be applied for physical, chemical, and microscopical analysis
of urine
161
162.
Automations in Urinalysis(cont….)
advantages of automations:
the readings are more reproducible and unbiased
help to analyze a great number of specimen in less
time
help to develop standards about the sediments and
give better interpretation about the sediments in
close agreement between laboratories
162
163.
Quality control inurinalysis.
Quality assurance is a set of activates starting
from specimen collection to issuing test results
that ensure test results are accurate and precise
as possible.
It is the sum of all the activates of the laboratory
that ensures test results are of good quality.
163
164.
Quality control inurinalysis cont’d…
Quality assurance includes
inside and outside the laboratory performance standards
good laboratory practice and management skills that are
required by achieving and maintaining a quality service and
that provide for continuing improvement
164
165.
Quality control inurinalysis (cont…)
• part of quality assurance, which primarily concern the
control of errors in the performance of tests and verification
of test results.
• must be practical, achievable, affordable, and above all
continuous.
• The purpose of quality control procedure is to monitor
analytical processes, analytical error and to correct result of
analysis.
165
166.
types of qualitycontrol programs
A) internal quality control
Is carried out in the laboratory, an intra-lab program.
encompasses all measurements made, technical skills performed
within an individual laboratory.
use control samples, like pooled serum
The purpose of quality control program is to insure tests are
performed reliably and reported correctly.
An effective quality control system detect errors at an early stage,
before they lead to incorrect test results.
• B) external quality control.
– External quality control is observation of variance in results when
the same material is analyzed in different laboratories
166
167.
Cont…..
B) external qualitycontrol.
External quality control is observation of variance in
results when the same material is analyzed in different
laboratories
Quality control steps:
Pre analytical steps
Analytical steps
Post analytical steps
167
168.
Pre analytical Qualitycontrol in urinalysis
read and understand requested paper
guide the patient to bring an appropriate urine sample
labeling the urine container after collecting the sample
cheek the material we are going to use whether they are properly
cleaned or not
ask the patient whether the urine sample has been long time ,more
than two hours, after it is voided.
do not accept contaminated requested paper
cheek the slide, the microscope, and all needed material before taking
the next procedure.
if the urine comes from far place ask or read the preservative applied
168
169.
Cot…
concentrate andfind out an abnormalities that is also related from
chemical and physical apperance.
proper sample preparation is also most important.
reduce possible source of errors
do not open the centrifuge while it is not stopped
proper balance of urine in the centrifuge
169
170.
analytical Quality controlin urinalysis
Small urine sample how to be rejected
follow exactly standard operation procedure (SOP)
Check and read reagent strip chemical test according to the instruction
of the manual of the manufacturer, at the right time
write the physical appearances properly
use the needed amount of urine for centrifugation
when discarding the supernatant, it has to be quick and vertical up side
down in order not to loss the sediment
examine as quickly as possible
170
171.
Post analytical Qualitycontrol in urinalysis
improper written result
incorrect calculation
missing of requesting paper
171
172.
172
Summary
• You shouldbe able to describe:
– Appearance and clinical significance of RBC and WBC.
– Appearance and clinical significance of three types of epithelial cells.
– Formation, composition and clinical significance of the different types of
urinary casts. types of crystals, identify them and state clinical significance of
each.
– Other formed elements to include: bacteria, fat, fibers, mucous, parasites,
sperm, starch, trichomonas and yeast.
– Types of quality assurance in urinalysis
173.
Exercise:
Say True orFalse
1.The number of casts preserved decrease as the pH of the urine
decreases.
2. Presence of RBCs in the urine is always indicative of a renal
disease.
3.Waxy casts are the end stage in the degeneration of cellular casts.
4. Pyuria refers to elevated numbers of leucocytes in the urine.
5.The presence of Bacteria in the Urine is determined using only
Microscope.
173
174.
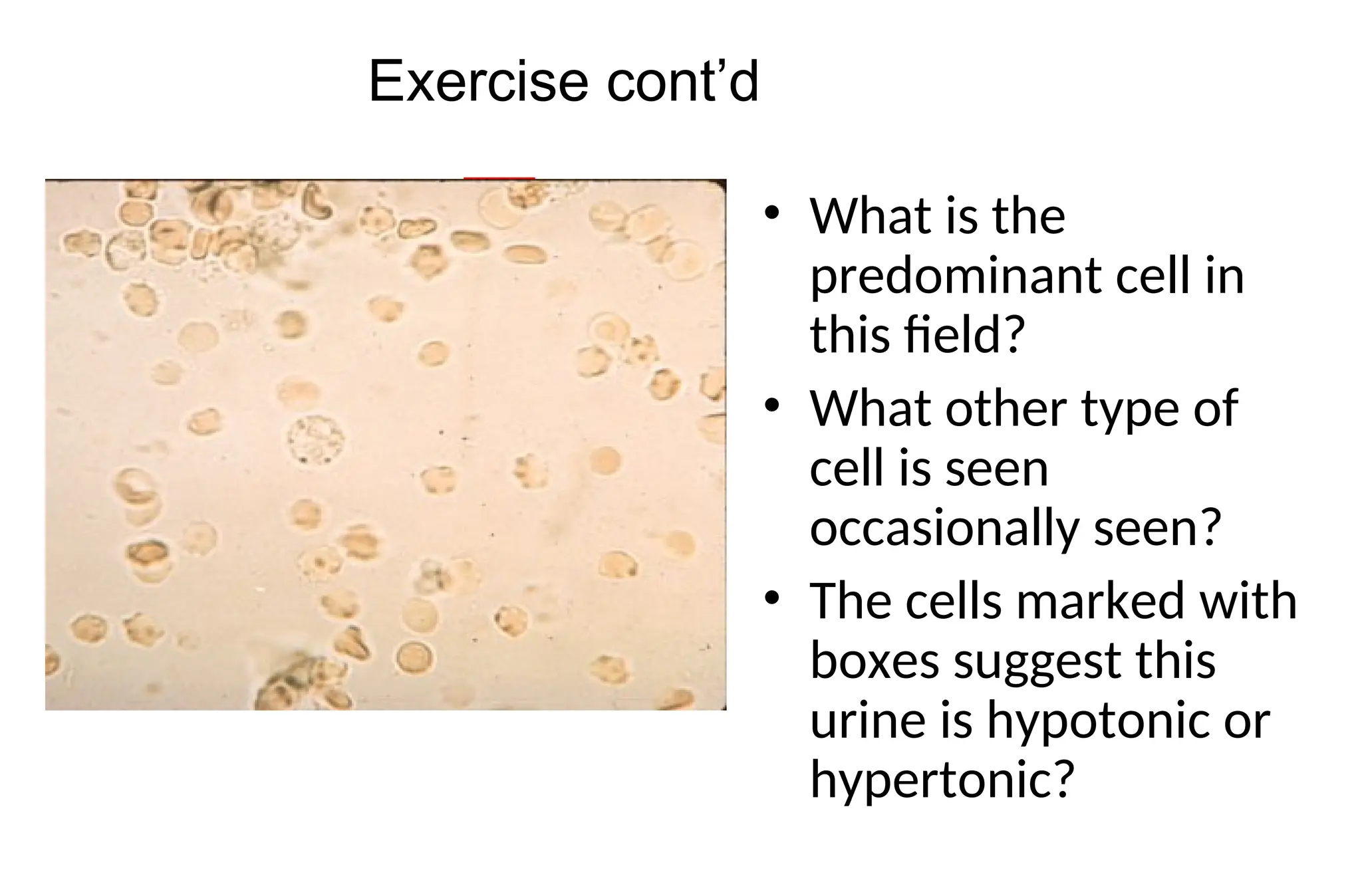
• What isthe
predominant cell in
this field?
• What other type of
cell is seen
occasionally seen?
• The cells marked with
boxes suggest this
urine is hypotonic or
hypertonic?
Exercise cont’d
References:
• District laboratorypractice in tropical countries. 2nd
ed. Part I. Monica
Cheesbrough, 2005
• Text book of urinalysis and body fluids. Doris LR, Ann EN, 1983
• Urinalysis and body fluids: A color text and atlas. Karen MR, Jean JL. 1995
• Clinical chemistry: Principles, procedures, correlation. 3rd
ed. Michael L. Bishop et
al. 1996
• Tietz Text book of clinical chemistry. 3rd
ed. Carl AB, Edward RA, 1999
• Clinical chemistry: Theory, analysis, correlation 4th
ed. Lawrence AK. 2003
• ASCP Document
• Urinalysis lecture note . Mistire W. , Dawite Y.
• Urinalysis and body fluids / Susan King Strasinger, 5th ed. 2008
178
Editor's Notes
#11 Note: If Pasteur pipette is not available, gently incline the tube and place drop of sediment into the clean, and dry slide.
#12 NOTE: Casts tend to concentrate near the edge of cover slide. For determination of cellular elements, casts, etc, the number of elements seen under at least 10 fields should be counted and the average of this number is used for report value. Other elements such as parasites are usually reported as well.
#18 RBCs will lyse in acetic acid while other elements will stay intact.
#20 Clinical significance
Presence of parasites, such as: Schistosoma hematobium
Presence of bacterial infection, such as: renal tuberculosis
Other disease conditions, such as hemophilia, malignant hypertension etc
#26 Note:possible to see single irregular nuclei and small round lobed nuclei in the WBCs, that are seen in the urine sediment
#32 * Knowing the origin of the epithelial cells and reporting it, may have more meaning when requested by the physician for special purpose, especially by the urologists. Thus routinely report only the presence of epithelial cells
#40 Interfering factors
Squameous epithelial cells from female patients that shade from vaginal area (together with vaginal discharge) may give false result of high epithelial cells.
#43 Researches indicated that the matrix of all casts is the high-molecular weight Tamm-Horsfall mucoproteins. During the formation of casts, different cellular elements may incorporated, & so various types of casts may formed based on the type of cellular element that they contains
#48 Hyaline casts are formed in the renal tubule consists largely of Tamm-Horsfall mucoprotein derived from renal epithelium.
Pure hyaline casts are devoid of formed elements.
Normal range: 0-2/HPF
Appearance
-Transparent (clear), cylindrical shape
- Have parallels side with slightly round ends
-Their appearance in urine depends on rate of urine flow, i.e. many hyaline casts are seen when the flow rate is slow, and are not seen in alkaline urine mostly; and as the degree of proteinurea is high, there concentration also increase.
#104 Additional filters can help to identify this.
#113 To check the presence or absence of bacteria a technician can either check for Nitrate that was formed in the urine after breakdown of nitrite into nitrate by the metabolic action of bacteria. most common cause of UTI and aerobic gram-negative bacilli, particularly, members of the enterobacteriacea, are the most dominant agents.
The Gram-positives account for proportionately large number of infections in hospital inpatients.
dipstick test can give indirect clue.
Further the observed bacterial cell can be identified by bacteriological culture
#115 Presence of bacteria may indicate the presence of UTI or contamination by genital or intestinal microflora.
To confirm what type of bacteria , culture them in appropriate media and perform biochemical tests for identification.
#122 Normally present in urine in different quantity.
Have pink to “brick red” color.
From very small granules and seen in cluster.
Dissolve in urine when the sample is gently heated.
When urine is left in the refrigerator, it shows heavy precipitation of urates.
#128 These crystals are pathologically present in ethylene glycol poisoning & severe chronic renal disease
#131 Sodium cyanide reduces cystine to cysteine & freed sulfhydryl groups will react with nitroprusside to form purple color. Because they are clinically significant, report as avg. # in 10 low power fields (lpf)
#154 Their presence in large amount with WBCs, may indicate UTI.
They may also act as a matrix on which minerals can be precipitated;thus,they may play a role in the genesis of calculus formation.
#155 They can be confirmed by logos iodine Pollen greens } - are seasonal.
Starch granules - incomplete digestion of starch
#156 Additional filters can help to identify this.
#159 Procedure
Add 1 or 2 drops of crystal violet safranin stain to approximately 1 ml of concentrated urine sediment. Mix and place a drop of this suspension on a slide and cover with cover slide
***It is commercially available as sedi-stain*** -a crystal violet safranin stain
#160 When such stains are used, it is recommended that both the stained and unstained sediment be mounted and observed, as the stain may cause precipitation of some constituents. This is especially the problem with alkaline urine specimens, because the precipitated materials may obscure important pathological constituents.
#161 Instruments, like Clinitek Atlas, after the urine sample is automatically pipette, different physical examination tests measured; specific gravity measured by the refractive index, the color is determined by measuring the color on a special reagent pad, transparency determined by measurement of transmitted and scattered light through the sample. instruments have been developed to electronically measure the intensity of the color reaction produced on the reagent strips.
The instruments are reflectance photometers. They measure the color that is produced by the chemical reaction between the analyte and the chemical impregnated on each testof the reagent strip.
The instruments contain a microprocessor that control and coordinates reflectance measurements at each test area.




![• This is a cast
containing ‘fat’
bodies, high
power
• On wet mount the
droplets are
highly refractile
[they bounce the
light back]
90](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-90-2048.jpg)

![133
Amino Acid Crystals
• Tyrosine
– fine, delicate needles,
colorless or yellow
– frequently in clusters or
sheaves [as in stacks of
wheat]
– see singly or in small groups
– in acidic urine
– less soluble than leucine, so
found more often](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-133-2048.jpg)
![134
Leucine
• Highly refractile yellow to brown
spheres in acid urine.
• Have concentric/radial striations
on their surface
• Can be mistaken for fat globules
[or vice versa]
• But will not stain with fat stains or
appear as maltese cross under
polarization
• Can be seen in urine containing
tyrosine crystals if use alcohol to
‘precipitate’
Bactrim has similar appearance
check patient history](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-134-2048.jpg)
![137
Confounding Conditions
• Diatrizoate meglumine [radiopaque contrast medium] can be
mistaken for cholesterol
– contrast medium will give abnormally high S.G. >1.040
– not associated with proteinuria or lipiduria
– cholesterol crystals found with normal S.G.
• Medications
– can be excreted in high concentrations, resulting in precipitation
– these crystals are termed ‘iatrogenic’
– proper identification of drug crystals important in alerting to
potential renal tubular damage](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-137-2048.jpg)
![140
• Sulfadiazine crystals appear
yellow to brown & as bundles of
wheat
– constriction may be central
or excentric
• Sulfamethoxazole [Bactrim &
Septra] more commonly seen
– brown rosettes or spheres
with irregular striations](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-140-2048.jpg)
![141
Radiographic Contrast Media
• Diatrizoate salts are used in IV contrast media
• Readily soluble in water & excreted in urine
• Diatrizoate meglumine [Renografin]
– crystals colorless, long pointed needles, singly or in clusters
or
– flat elongated rectangular plates
• distinguished from cholesterol by large # present & high
S.G. [>1.040]
• lack significant proteinuria & lipiduria
• diatrizoate appears in acidic urine up to 4 hrs post injection
– can cause false pos. sulfosalicylic acid test](https://image.slidesharecdn.com/chapterfive-250514050014-d6afba1d/75/Chapter-five-ppt-URINE-ANALYSIS-EXAMINATION-141-2048.jpg)