This document provides guidance on the management of upper gastrointestinal bleeding (UGIB). It outlines the following key points:
1. Initial steps include assessing hemodynamic stability, IV access, monitoring, fluid resuscitation, and basic lab tests. Endoscopy within 24 hours is critical for diagnosis and treatment.
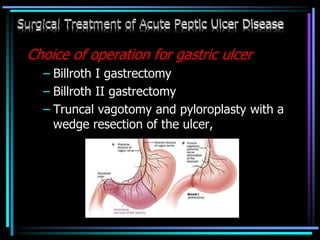
2. For non-variceal bleeding, endoscopic therapies like injection, thermal coagulation, and clipping are first-line. Refractory or high-risk bleeding may require surgery.
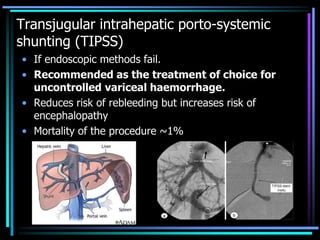
3. Variceal bleeding requires urgent endoscopic ligation or sclerotherapy. Transjugular intrahepatic portosystemic shunting or surgical shunting may be needed if initial measures

















































































![Fatty liver disease with Diabetes Mellitus [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/fattyliverwithdmfinal-160520141759-thumbnail.jpg?width=640&height=640&fit=bounds)

![Adult immunization [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/adultimmunization-160520135511-thumbnail.jpg?width=640&height=640&fit=bounds)





















