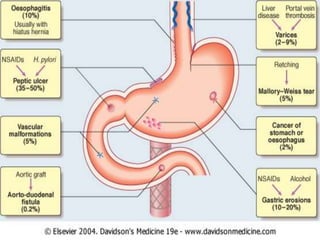
Upper gastrointestinal bleeding (UGIB) is a potentially life-threatening emergency caused by bleeding in the esophagus, stomach, or duodenum. Common causes include esophageal/gastric varices, ulcers, cancers, and esophagitis. Signs include hematemesis, melena, and hematochezia. Initial treatment involves stabilizing the patient, identifying the source of bleeding through endoscopy, and administering treatments like band ligation, injection therapy, or anti-secretory drugs. Surgery may be required for persistent or recurrent bleeding after other measures fail.