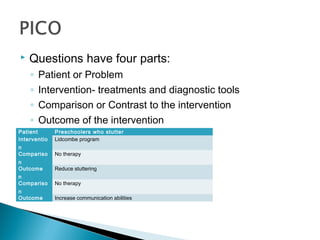
This document discusses evidence-based practice in speech-language pathology. It defines evidence-based practice as integrating clinical expertise, patient values, and the best research evidence. Lower levels of research evidence are still useful if they are the best available. Treatment efficacy focuses on controlled studies while effectiveness looks at outcomes under typical clinical conditions. Clinicians should have an open and honest approach when considering different treatment options and be guided by principles of beneficence, autonomy, nonmaleficence, and justice. Forming answerable clinical questions is important to evidence-based practice.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




