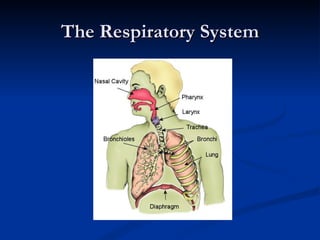
The document summarizes the process of respiration and its role in voice production. It describes the three main components of voice production - respiration, phonation, and resonance. It then focuses on respiration, explaining the respiratory system and how inspiration and expiration work through changes in air pressure and muscle actions. It notes how respiration differs for speech compared to rest, using more forceful inhalation and longer exhalation while speaking.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










