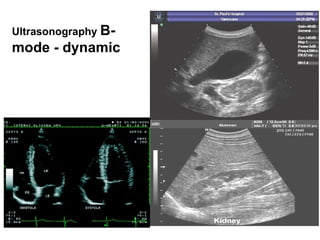
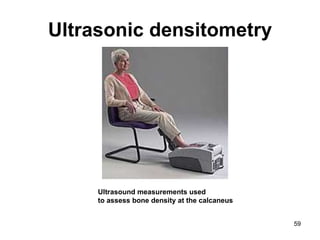
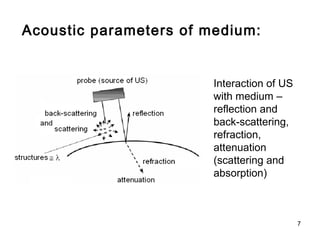
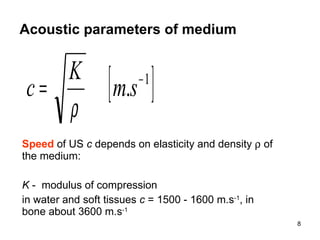
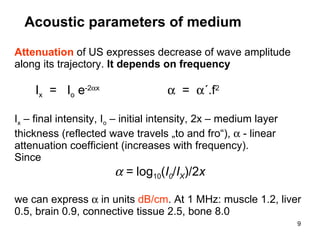
This document provides an overview of ultrasound diagnostics and various ultrasound imaging techniques. It begins with a brief history of ultrasound diagnostics and outlines common ultrasound modalities including ultrasonography (A, B, and M modes), Doppler flow measurement, tissue Doppler imaging, and ultrasound densitometry. The document then discusses physical properties of ultrasound, acoustic parameters of tissues, and interactions of ultrasound with tissues. It provides details on various ultrasound imaging modes and techniques such as B-mode, M-mode, harmonic imaging, and 3D imaging. The document also covers Doppler blood flow measurement principles and different Doppler methods including duplex, color Doppler, and triplex.

![Acoustic parameters of medium Attenuation of ultrasound When expressing intensity of ultrasound in decibels, we can see the amplitudes of echoes to decrease linearly . depth [cm] I or P [dB] attenuation](https://image.slidesharecdn.com/ultrasounddiagnostics-fin-110914111504-phpapp02/85/Ultrasound-diagnostics-fin-10-320.jpg)