The document discusses digital subtraction angiography (DSA), a medical imaging technique used to visualize blood vessels. It provides an overview of the history and development of DSA, including key contributors and technological advances. Some of the main points covered include:
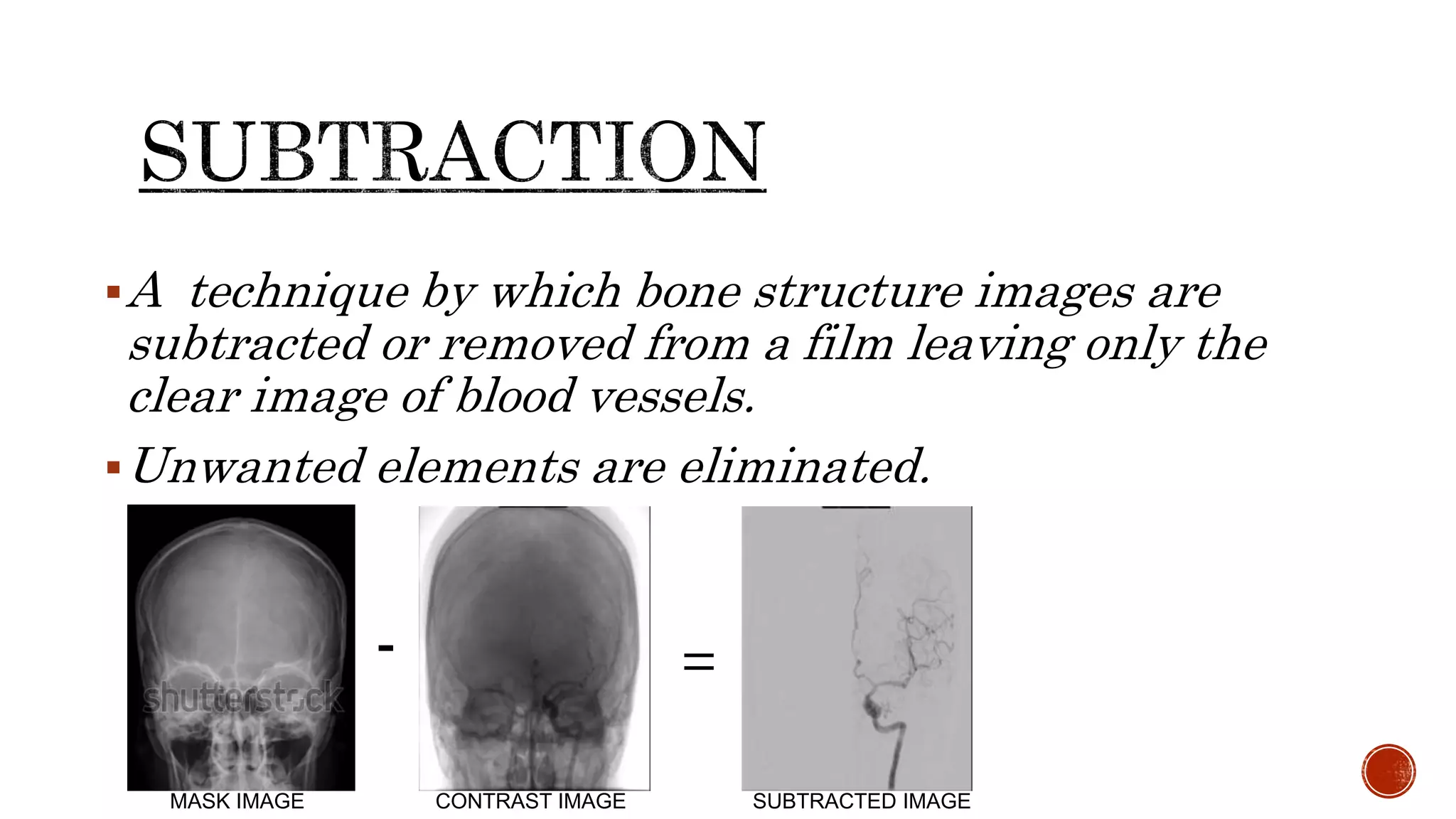
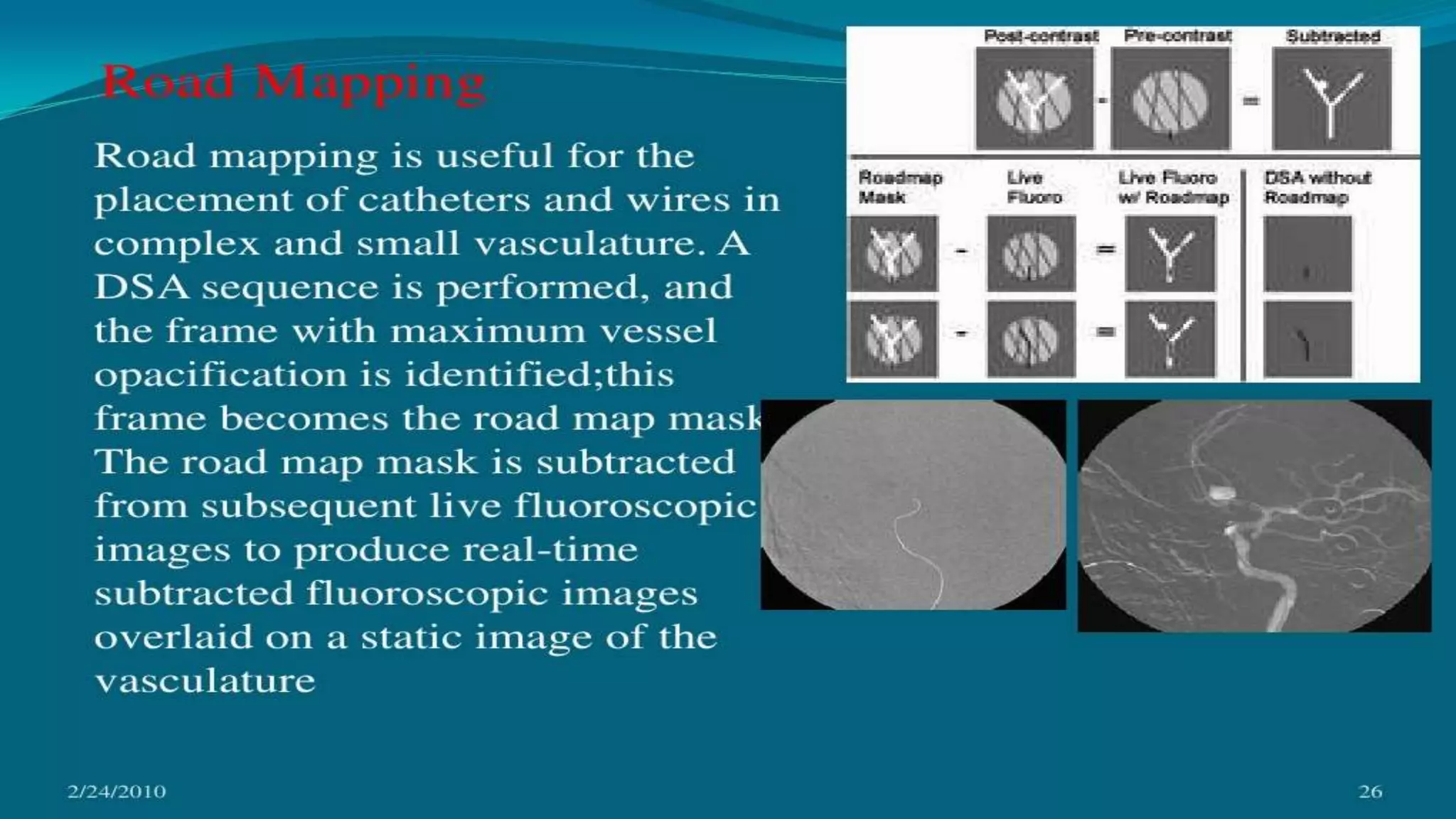
- DSA involves injecting contrast dye and digitally subtracting bone structures from images to clearly depict blood vessels
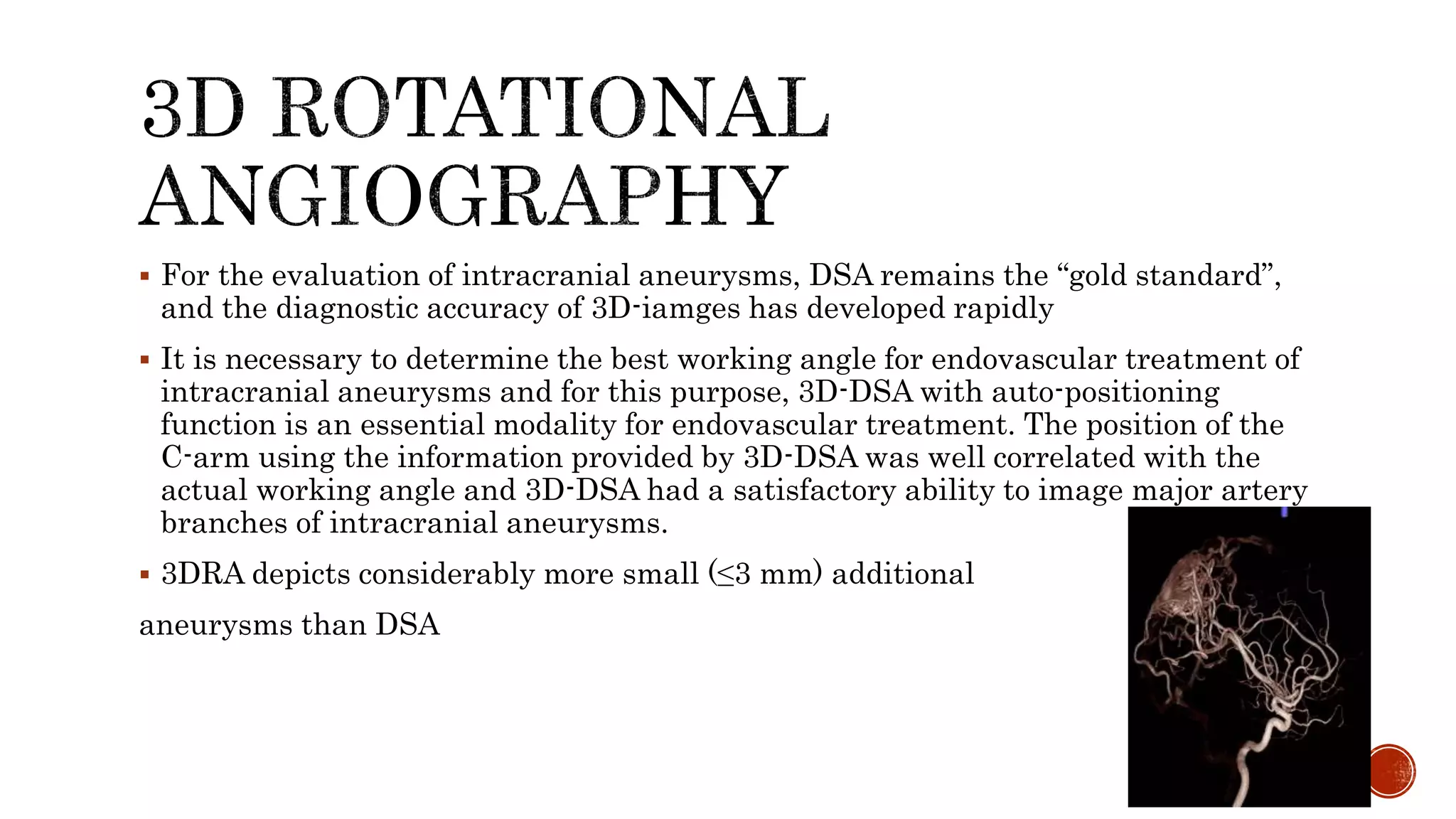
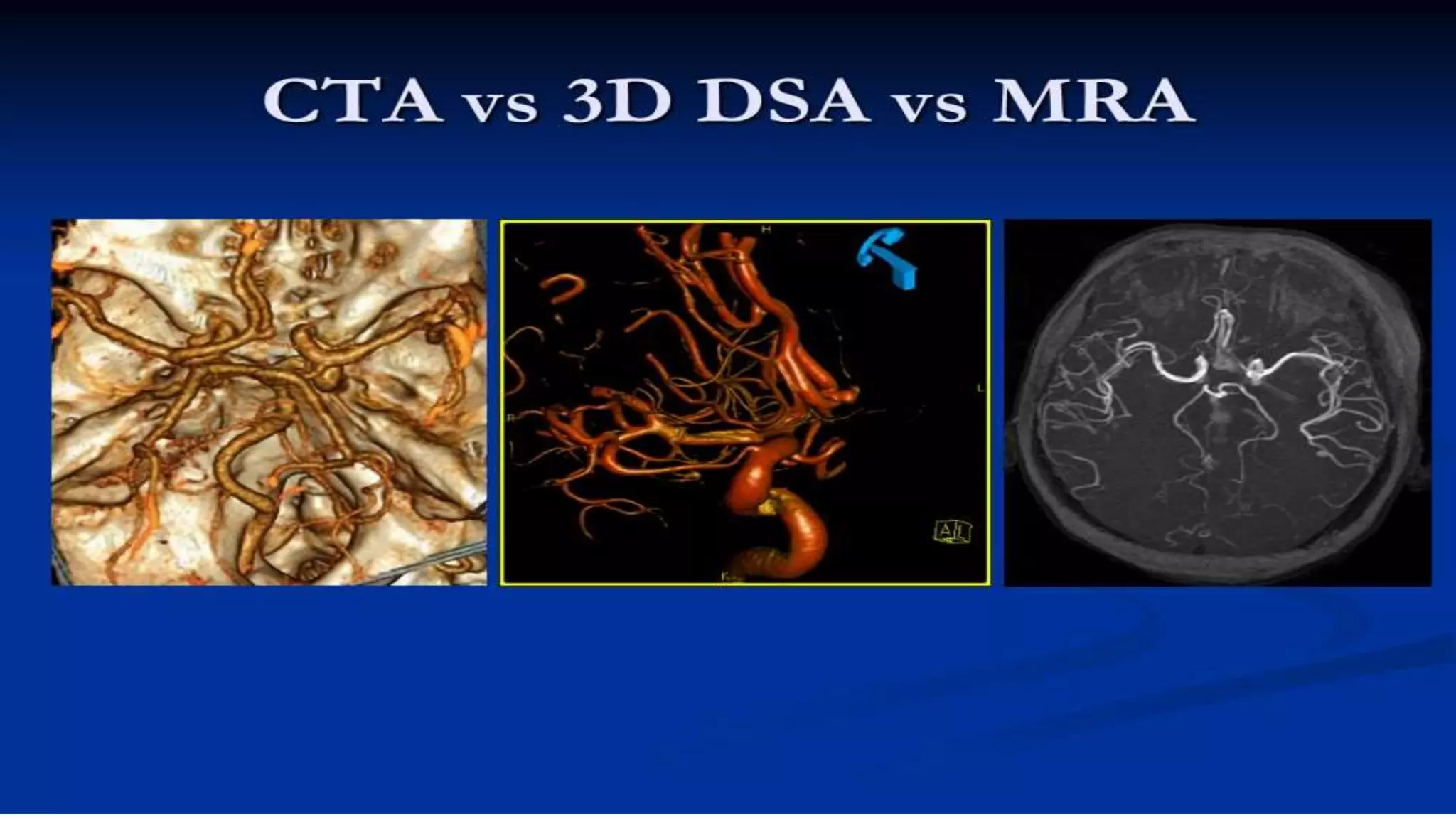
- It has been improved over time through the introduction of techniques like dual energy subtraction, temporal filtering, and more recently 3D and 4D DSA
- Advances like these have helped increase diagnostic accuracy for evaluating conditions like intracranial aneurysms