- Burns are a leading cause of injury in children, with scalds being the most common type especially in young children. Thorough history is important to identify potential abuse.
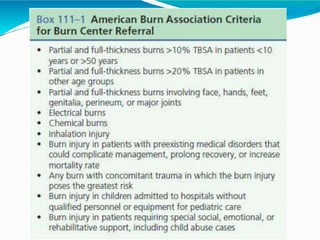
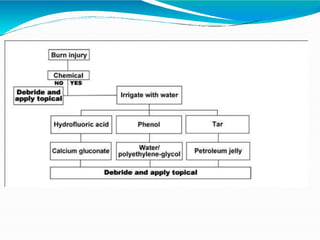
- Early management focuses on stopping the burning process, assessing airway status, estimating burn size, starting fluid resuscitation, and providing pain control. Large or full thickness burns may require inpatient care.
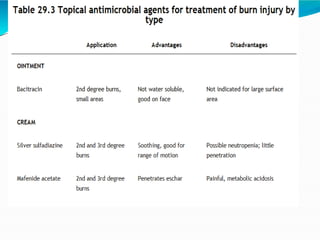
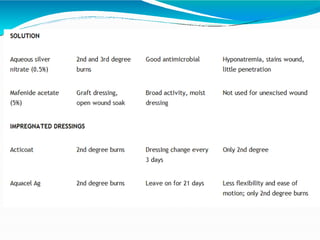
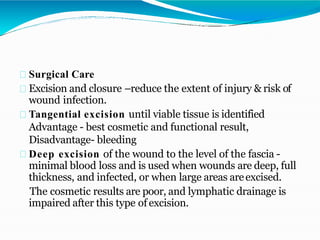
- Fluid resuscitation follows the Parkland formula to replace losses and maintain circulation. Ongoing wound care aims to prevent infection while the burns heal. Inhalation injuries require careful monitoring and pulmonary support.