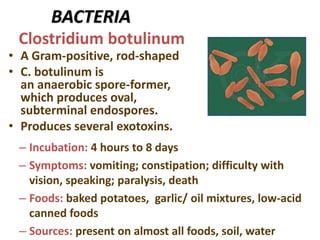
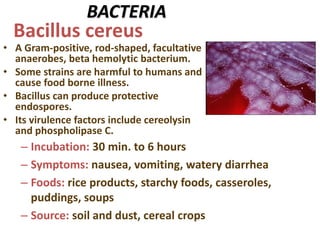
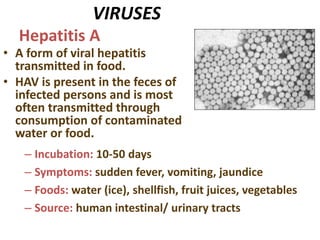
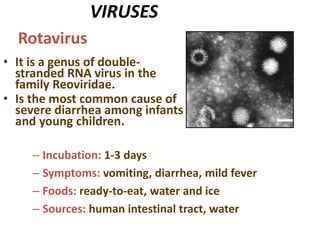
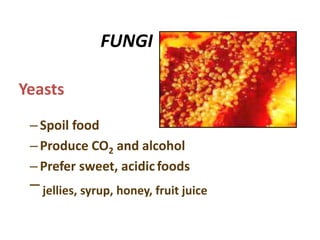
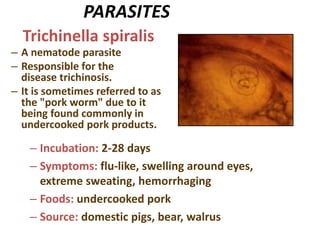
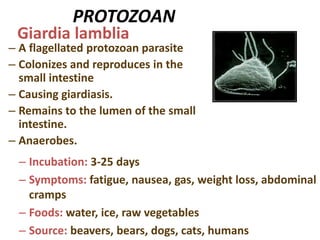
Food poisoning is caused by consuming contaminated food or water and can be caused by bacteria, viruses, parasites, toxins, or chemicals. It is a major global health issue resulting in millions of cases and deaths each year. Food poisoning is generally classified as food-borne infections, caused by pathogens invading the intestines, or food-borne intoxications, caused by preformed toxins in food. Common causes of food poisoning include Salmonella, E. coli, C. botulinum, S. aureus, and viruses like hepatitis A and rotavirus. Symptoms include diarrhea, vomiting, abdominal cramps, and fever. Treatment focuses on rehydration and electrolyte replacement. Prevention involves proper food handling and hygiene practices.


































![Food_poisoning[2].pptx it explain about how food poisoning is caused , how i...](https://cdn.slidesharecdn.com/ss_thumbnails/foodpoisoning2-250714162601-7fdcf1b4-thumbnail.jpg?width=640&height=640&fit=bounds)































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
