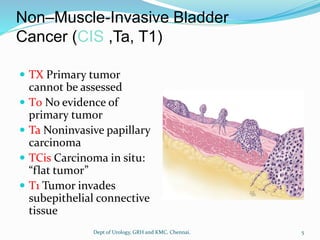
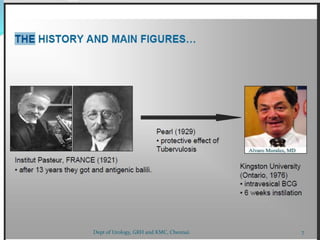
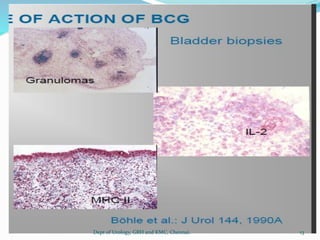
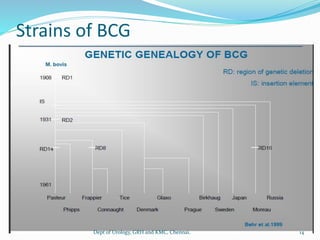
This document discusses treatment options for non-muscle invasive bladder cancer, including transurethral resection of bladder tumor (TURBT), bacillus Calmette-Guerin (BCG) immunotherapy, and intravesical chemotherapy. It provides details on the administration and schedule of BCG, lists its contraindications and potential side effects, and discusses options for patients who fail or are intolerant to BCG therapy, including interferon and investigational immunotherapies.




























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)