Downloaded 11 times















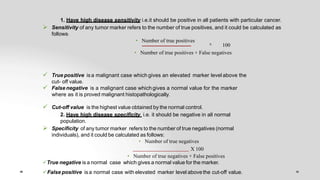

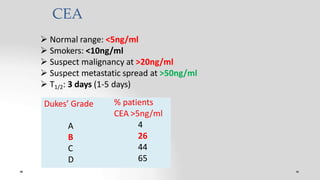
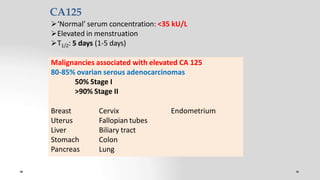
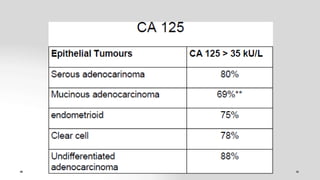
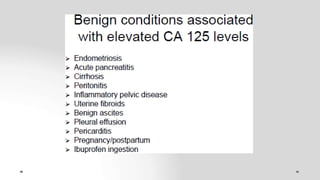






Tumor markers are substances produced by tumor cells or the body's response to tumors that can be detected in blood, urine, or tissue. They are used to screen for cancers, help diagnose cancer, determine prognosis, detect recurrence, and monitor treatment response. An ideal tumor marker would be highly sensitive and specific to a particular cancer, correlate with tumor size, respond rapidly to treatment, and predict recurrence before clinical detection. Examples of commonly used tumor markers include AFP, CEA, CA125, PSA, and CA15-3. Their levels can be elevated in both cancer and some benign conditions.























































































