Downloaded 163 times
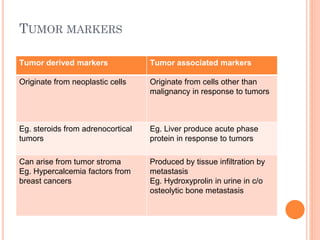

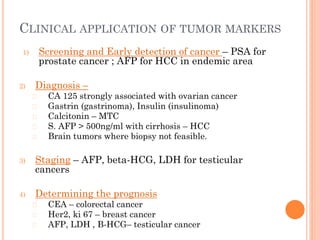
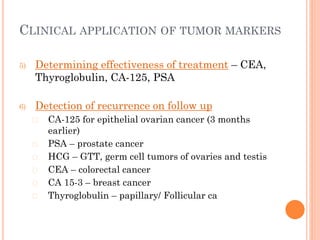


Tumor markers are substances produced by cancer cells or other cells in response to cancer that can be detected in bodily fluids or tissues. The ideal tumor marker would be highly sensitive and specific to a cancer, produced early in cancer progression, and correlated with tumor burden. Common tumor markers include AFP for liver and germ cell cancers, CEA for gastrointestinal cancers, PSA for prostate cancer, CA125 for ovarian cancer, and calcitonin for thyroid cancer. Tumor markers have applications in cancer screening, diagnosis, staging, determining prognosis, monitoring treatment response, and detecting recurrence.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





