Downloaded 257 times
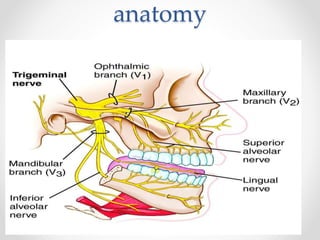
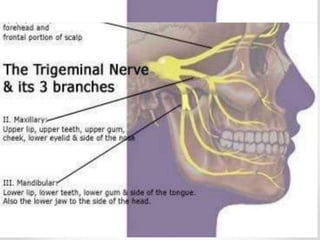
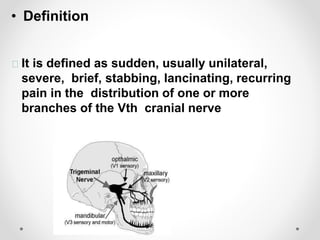

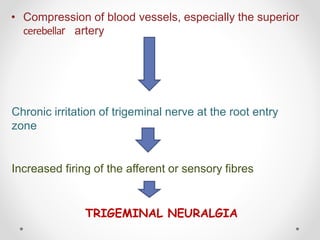
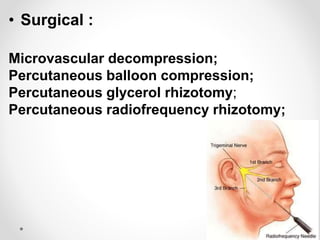


Trigeminal neuralgia is a condition characterized by severe, stabbing, recurrent facial pain that affects one or more branches of the trigeminal nerve. It is often triggered by mundane activities like eating or shaving. The most common cause is compression of the trigeminal nerve root by blood vessels. Treatment involves medications like carbamazepine or surgical procedures to decompress the nerve. Differential diagnoses include dental pain, sinusitis, and migraines.



































































