




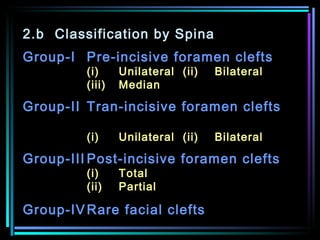
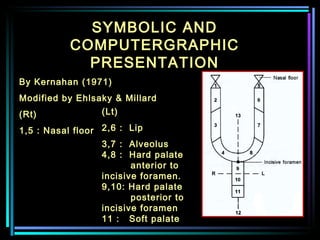


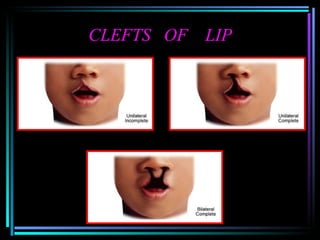



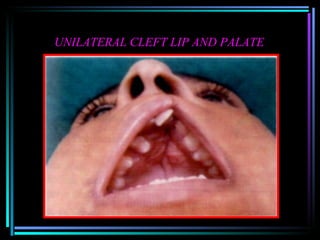






This document summarizes a seminar on cleft lip and palate. It discusses the development, etiology, classification, incidence, clinical features, and associated syndromes of cleft lip and cleft palate. Various theories for the development are provided. Genetic and environmental factors that may cause clefts are described. Different classification systems for clefts are outlined, including those based on morphology and embryology.






























































































