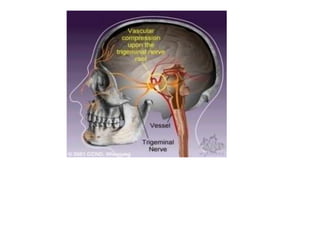
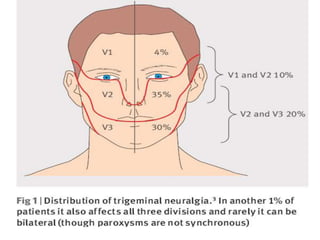
This document discusses trigeminal neuralgia, a condition characterized by severe, stabbing facial pain. It causes sudden, brief attacks of pain along the distribution of the trigeminal nerve. Common causes include compression of the trigeminal nerve root by blood vessels. Symptoms include unilateral pain in the jaw, cheek, forehead, or around the eye that is triggered by mundane activities like eating or talking. Diagnosis involves patient history and neurological exam. Treatment options include carbamazepine, phenytoin, or surgery to decompress the trigeminal nerve if medications do not provide relief from the stabbing facial pain.