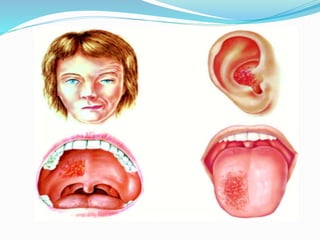
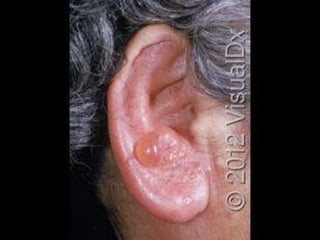
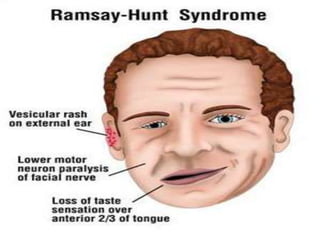
Ramsay Hunt syndrome is caused by reactivation of the varicella zoster virus, which causes chickenpox, in the facial nerve ganglia near the ear. This causes a rash around one ear and facial paralysis on the same side. It affects cranial nerves 7 and 8, resulting in symptoms like facial weakness, hearing loss, and pain. Treatment involves antiviral drugs to treat the infection along with steroids to reduce inflammation. Prognosis is better if treatment begins within 3 days and for children compared to adults. Early diagnosis and treatment improves chances of recovery from facial paralysis.