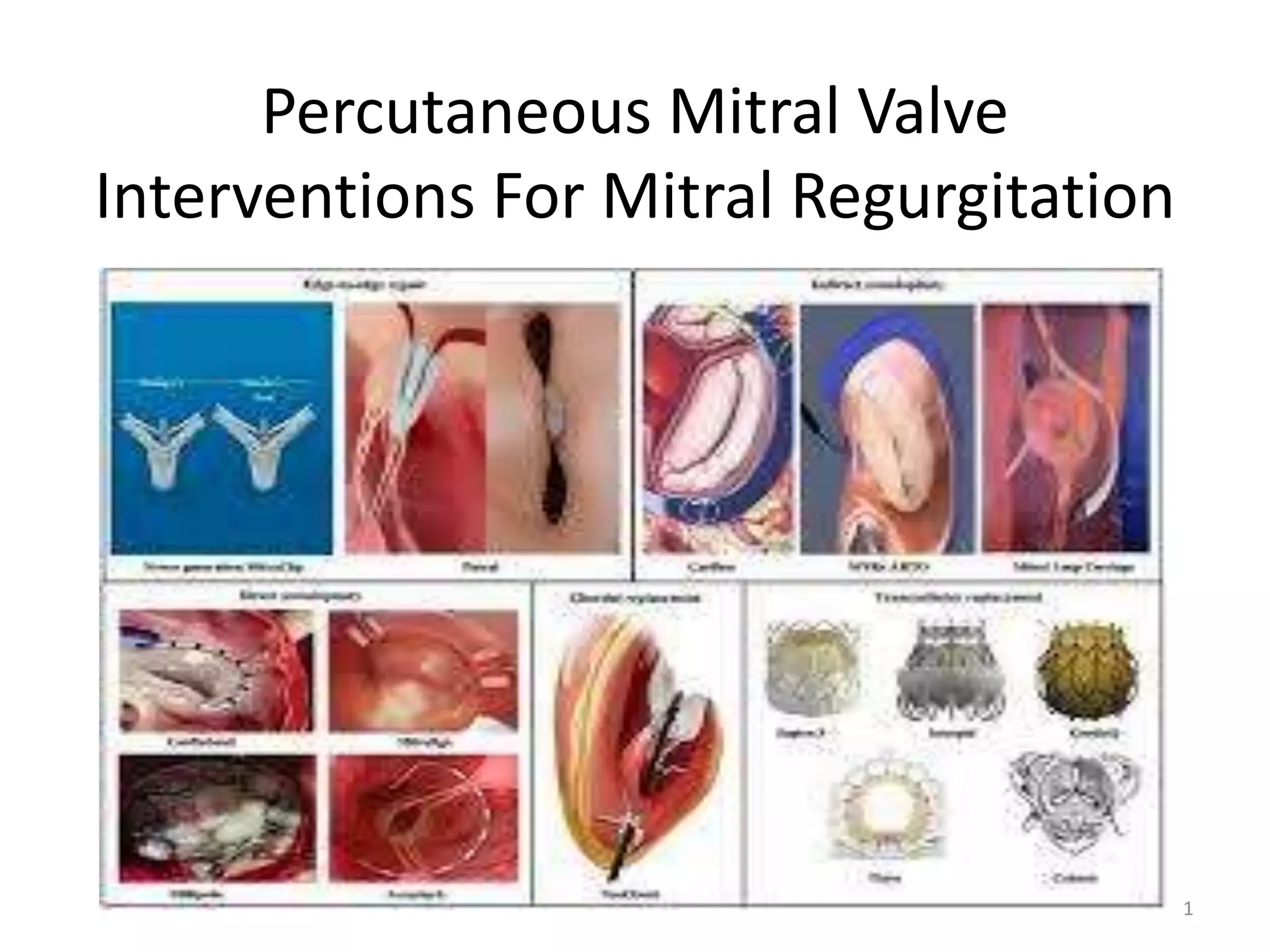
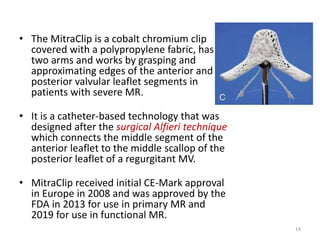
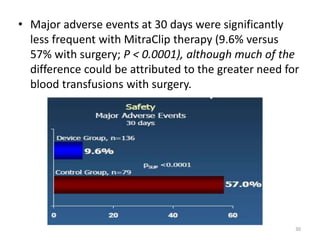
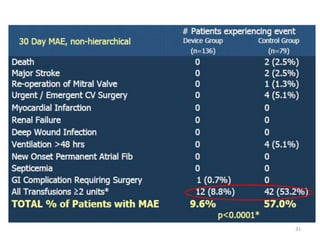
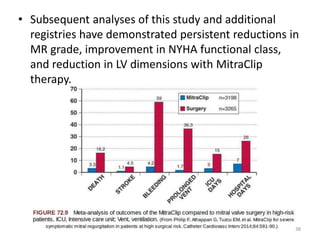
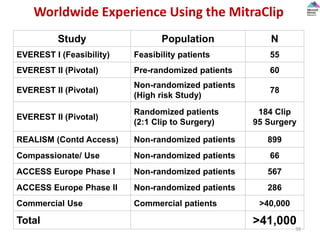
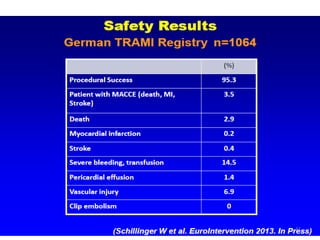
This document discusses percutaneous mitral valve interventions for mitral regurgitation. It begins by describing the anatomy of the mitral valve and causes of mitral regurgitation. It then discusses the natural history of mitral regurgitation and indications for surgery. Current percutaneous options are described including the MitraClip device, which is the only FDA approved one. The MitraClip procedure involves grasping the leaflets edges to reduce regurgitation. Early results show high rates of procedural success for MitraClip in patients at high risk for surgery. Complications are usually low at 15-19% and include bleeding, partial clip detachment, and stroke.



![• Clinical feasibility was evaluated using the next-generation
CARILLON XE device in 48 patients with FMR and LV systolic
dysfunction.
• The device was successfully implanted in 30 patients.
• At the 6-month follow-up, there was a durable and
significant decrease in
– mitral annulus diameter (from 4.2 to 3.78 cm [10%]),
– MR (average reduction, 23%), and
– NYHA class (from 2.9 to 1.8), and
• Improvement in the quality-of-life score and 6-minute walk
testing (from 307 to 403 meters).
AMADEUS trial
(CARILLON Mitral Annuloplasty Device European Union Study)
69](https://image.slidesharecdn.com/percutaneousmitralvalveinterventionsformr-yogesh-200305160230/85/Percutaneous-mitral-valve-interventions-for-MR-69-320.jpg)





























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















