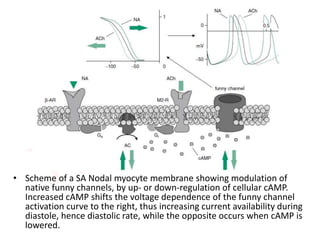
The funny current, also known as the If current or pacemaker current, underlies the generation of the diastolic depolarization phase of the cardiac action potential and is responsible for repetitive cardiac activity. It is a mixed sodium/potassium current that is activated during membrane hyperpolarization in the diastolic range. The If current is modulated by intracellular cyclic AMP levels and its main channel subunits are HCN channels. Ivabradine is a specific inhibitor of the If current that reduces heart rate by decreasing the slope of diastolic depolarization without substantially changing action potential duration.