Downloaded 13 times

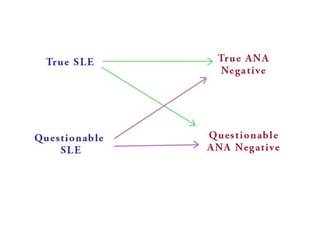
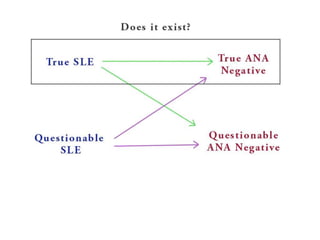

The document reviews two articles discussing antinuclear antibody-negative lupus. The first article from 2004 found that in most reported cases of supposed ANA-negative lupus, the diagnosis of lupus was questionable or ANA negativity could not be definitively established. The second article from 2018 similarly found that true ANA-negative lupus is extremely rare, occurring in less than 2% of reported cases, once technical issues and confounding factors are accounted for. The document concludes that true ANA-negative lupus is now predominantly a historical phenomenon rather than a distinct entity.