Download to read offline



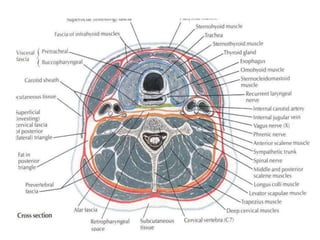










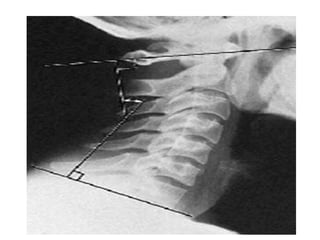










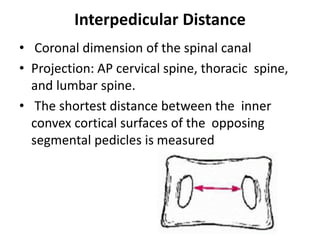

























































































This document provides descriptions and guidelines for evaluating various radiographic lines and angles in the cervical, thoracic, and lumbar spine. It discusses anatomical structures like the retropharyngeal space and various methods for assessing spinal alignment, curvature, disc height, intervertebral angles, spinal canal dimensions, and detecting instability. Key measurements mentioned include Cobb's angle for scoliosis, Torg ratio for cervical stenosis, Ruth Jackson's lines for cervical flexion/extension stress, and Van Akkerveeken's measurement for lumbar instability. The document serves as a reference for radiologists and clinicians to evaluate common spinal radiographic findings.



































































