Downloaded 19 times
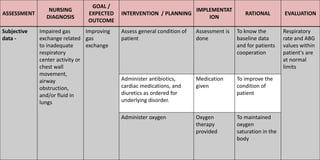
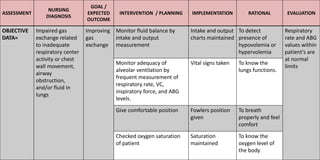
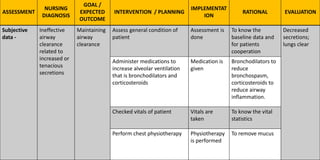
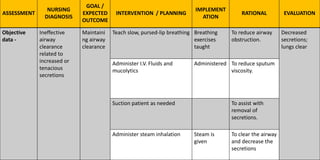
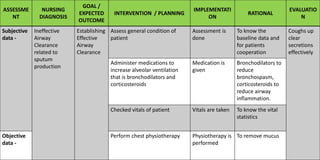
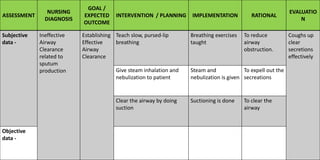
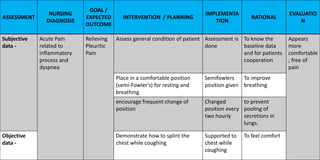
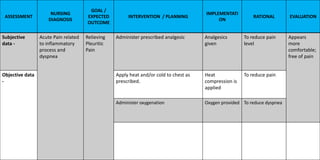
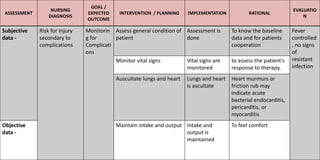

The document outlines a comprehensive nursing care plan for respiratory system assessment, highlighting the evaluation of breathing patterns, oxygen levels, and potential complications. It includes nursing diagnoses related to gas exchange, airway clearance, and pain management, along with proposed interventions such as medication administration and physiotherapy. The goal is to improve patient outcomes through careful monitoring and tailored treatments based on specific assessments.























































































