1. A tooth supported overdenture is a removable partial or complete denture that covers and receives support from one or more remaining natural teeth or dental implants.
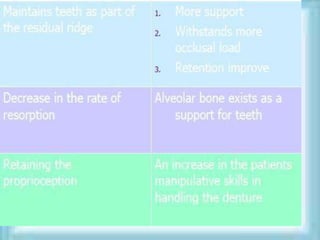
2. It provides advantages like ridge preservation, improved retention, stability and support compared to conventional complete dentures.
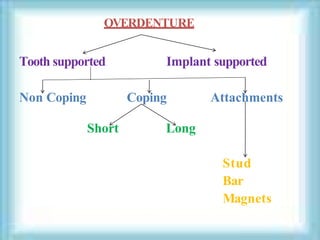
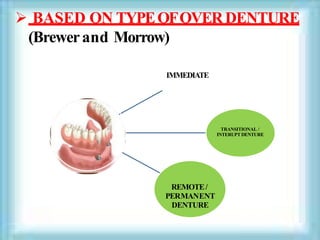
3. Tooth supported overdentures can be classified based on the type of abutment preparation (coping vs non-coping) and the timing of placement (immediate, interim or definitive).







































![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)














































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















