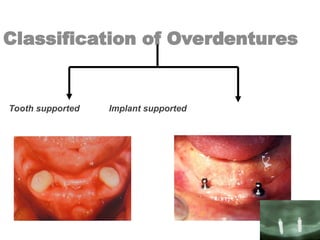
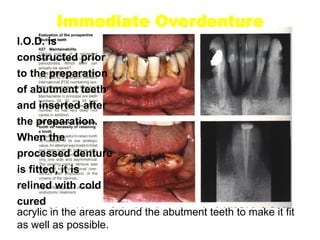
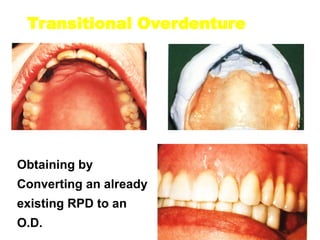
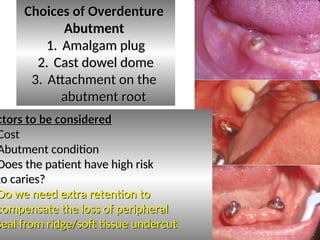
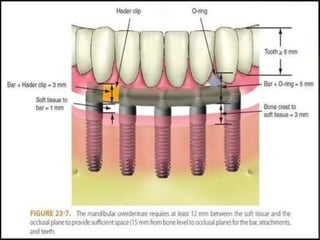
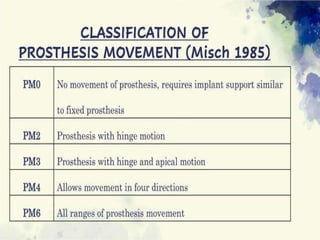
The document discusses overdentures, which are prosthetics constructed over existing dental structures, offering advantages like preservation of bone, improved occlusal stress distribution, and patient acceptance. It details the types, classifications, and indications for overdentures, along with their advantages and disadvantages, emphasizing their psychological benefits and converting existing dentures. Additionally, it describes clinical procedures for overdenture treatment planning and emphasizes the importance of proper abutment selection and maintenance for successful outcomes.