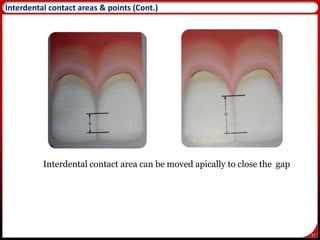
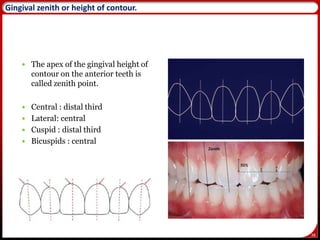
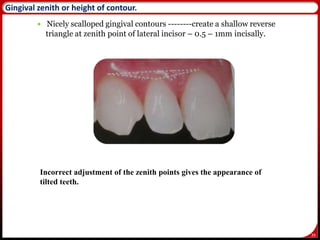
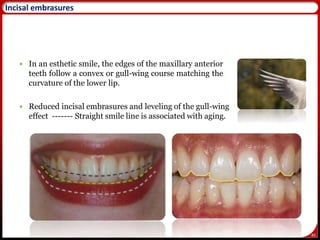
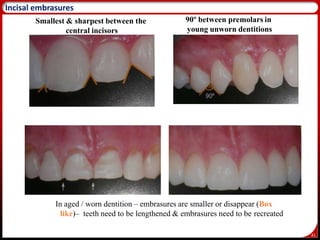
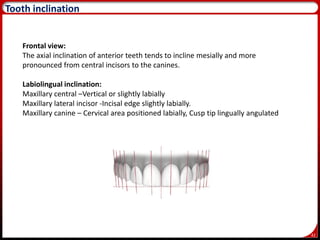
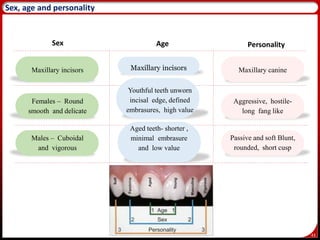
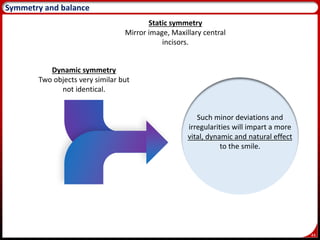
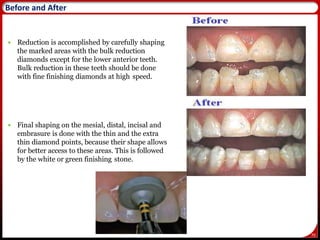
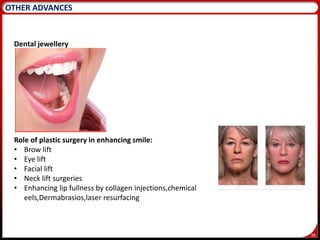
The document discusses various aspects of smile design and esthetics. It begins with definitions of esthetics and smile design. It then covers components of an esthetic smile including facial components like lips and dental components like teeth and gingiva. It describes classifications of smiles and properties of color. It also discusses topics like shade selection, esthetic treatment planning, contouring of teeth, and recent advances in smile design.