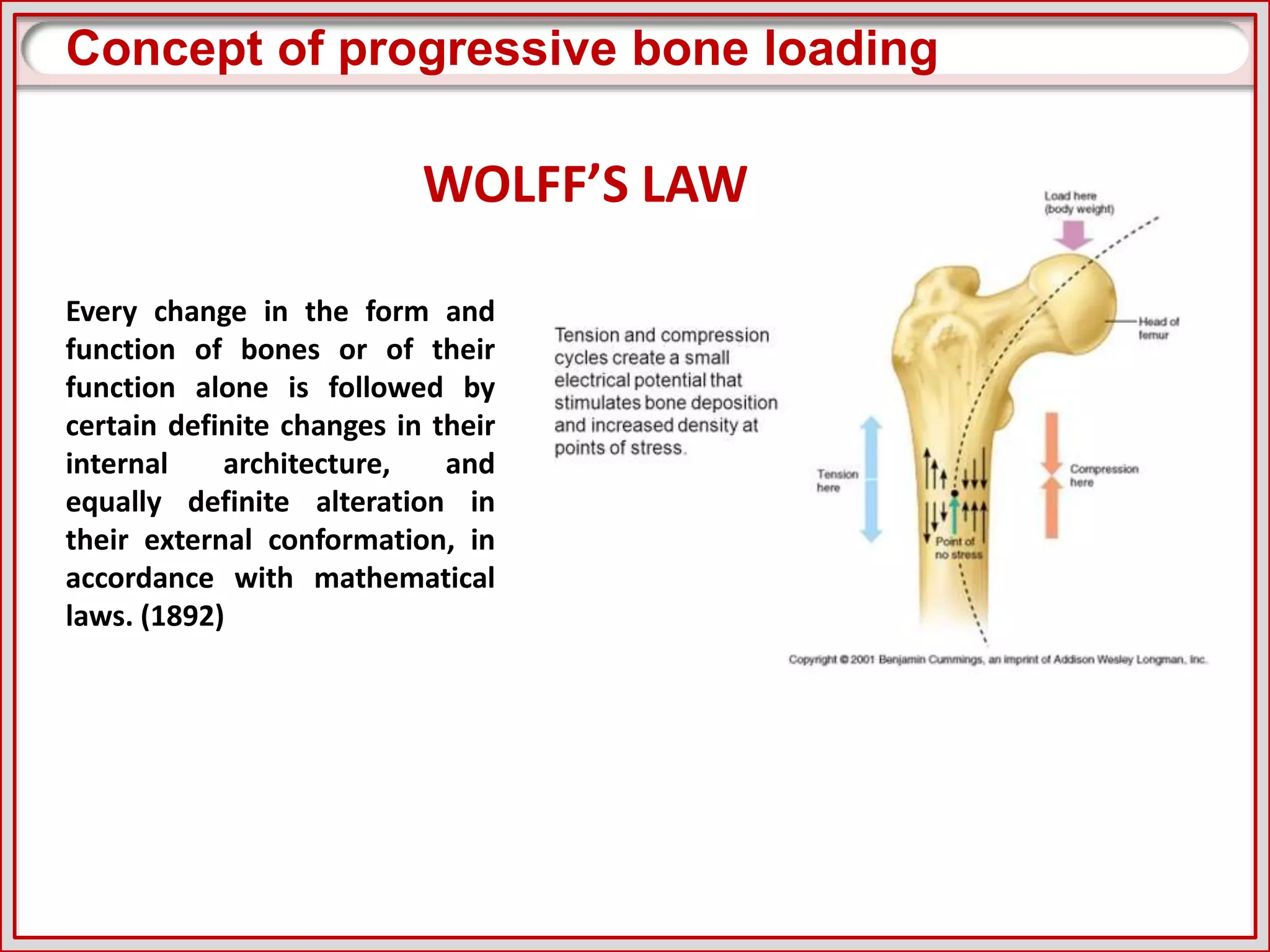
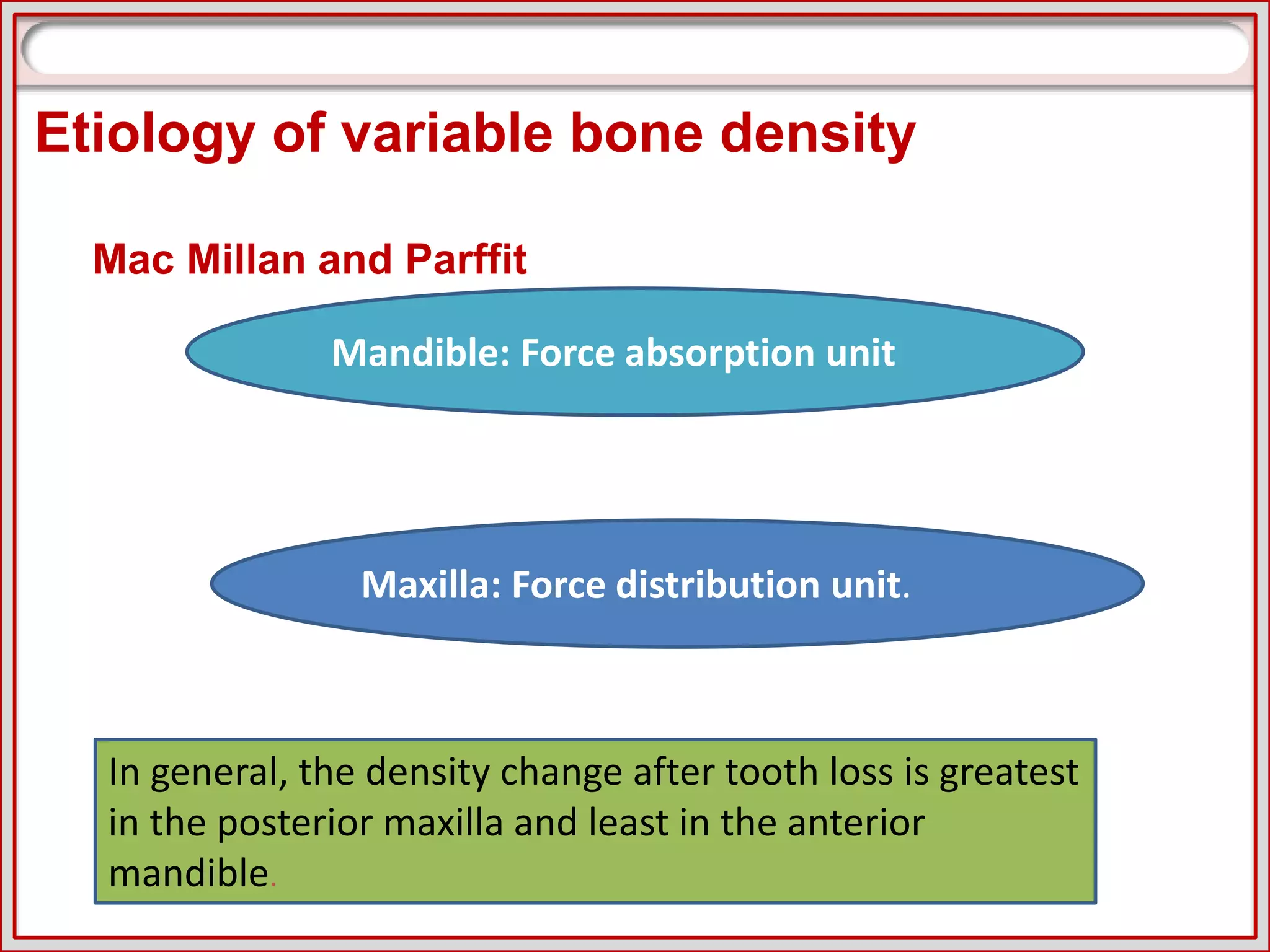
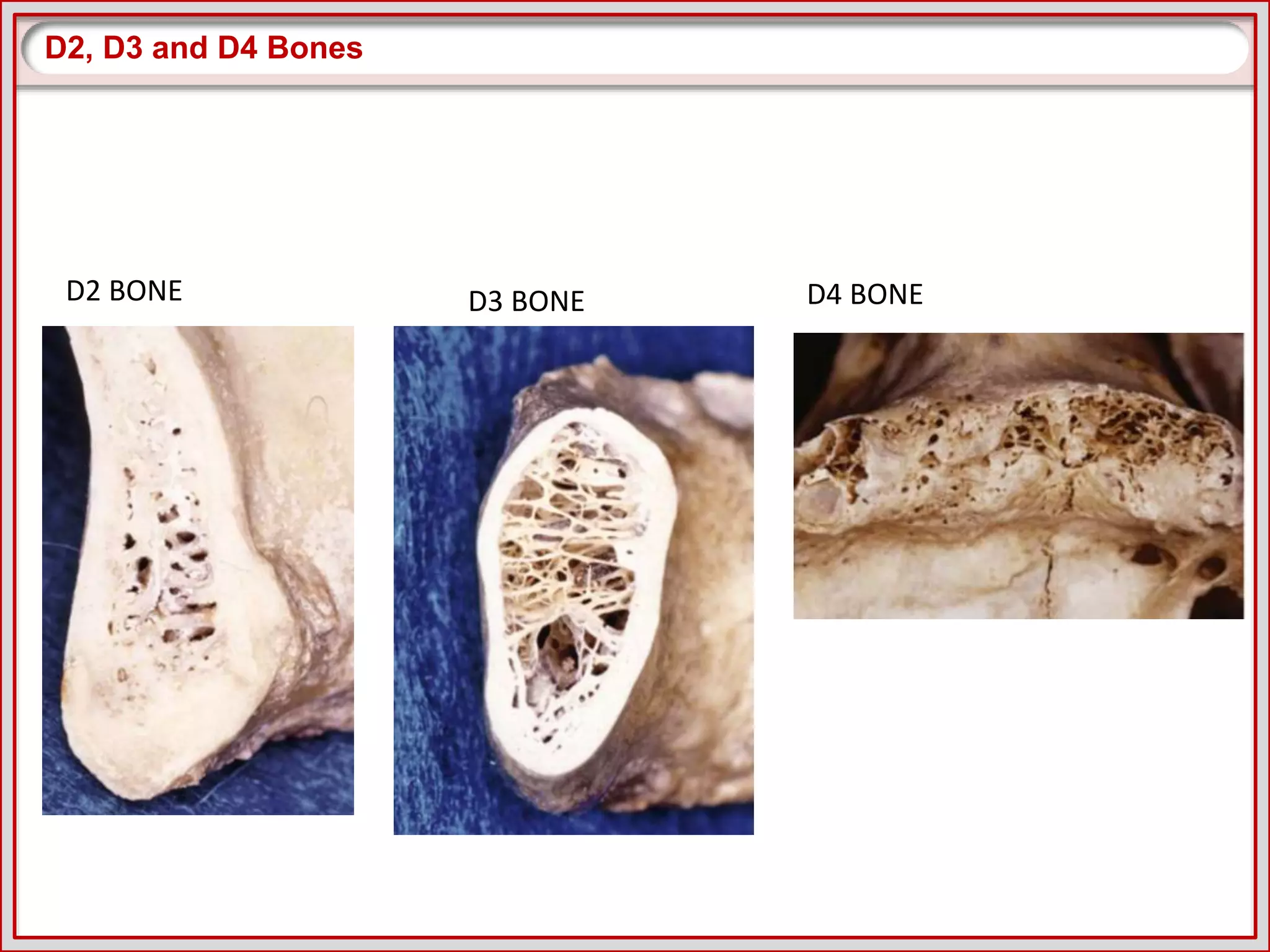
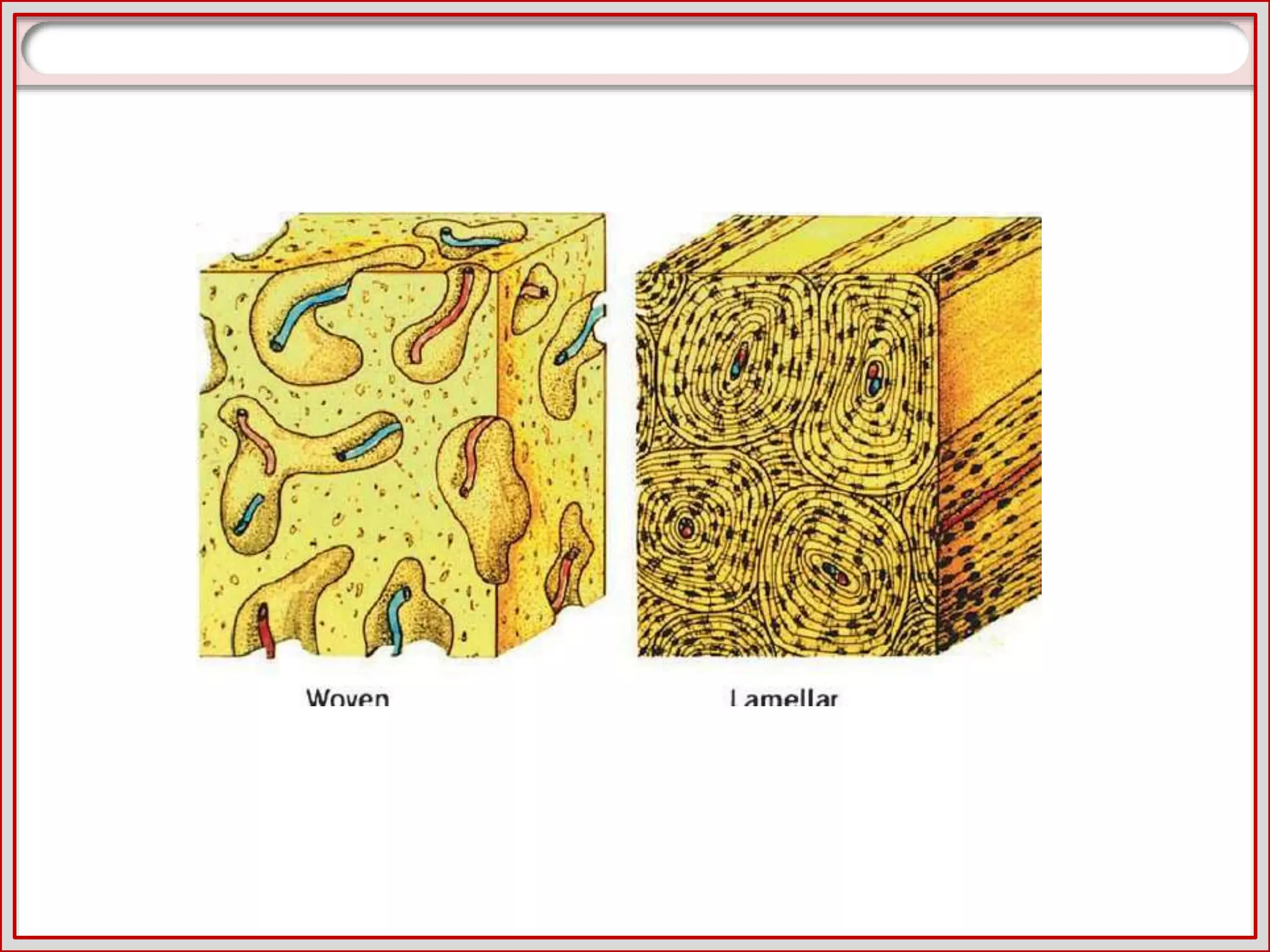
This document discusses progressive bone loading for dental implants. It begins with an introduction and table of contents. Then it discusses concepts like bone density classifications, rationale for progressive loading based on studies showing bone adapts to stress over time. It outlines elements of progressive loading protocols including extended healing times based on bone density, use of provisional restorations to gradually load bone, and diet restrictions. Studies supporting progressive loading show less crestal bone loss and increased bone density around loaded implants. The conclusion is that progressive loading aims to strengthen bone and reduce risk of implant failure.







































































































![Bone Density.pptxdfrftu890-/897\]lpjkgfds](https://cdn.slidesharecdn.com/ss_thumbnails/bonedensity-251027073618-7a77a65b-thumbnail.jpg?width=640&height=640&fit=bounds)












































