Overdenture
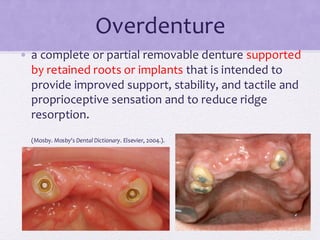
• a completeor partial removable denture supported
by retained roots or implants that is intended to
provide improved support, stability, and tactile and
proprioceptive sensation and to reduce ridge
resorption.
(Mosby. Mosby's Dental Dictionary. Elsevier, 2004.).
• Complete denturewearers suffered irreversible
bone loss especially in the first year.
• The rate in the mandible being four times than the
maxilla.
• In complete denture wearers, the average alveolar
ridge reduction in 25 years
• lower anterior : 9 – 10 mm
• Upper anterior : 2.5 - 3.0 mm
(Atwood and Tallgren 1972)
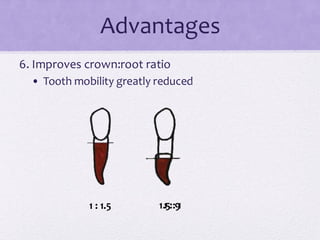
Advantages
1. Preservation ofridge form and alveolar bone.
Radiographic study to compare bone loss
showed that patients with complete
overdentures at canine had less bone
resorption compared patients with
complete dentures only.
Gerodontology 25 (2008) 118-123
11.
Mandibular overdenture preservealveolar bone
in the mandible by 8 times compared to
conventional dentures.
(Crum RJ, Rooney GE 1978)
12.
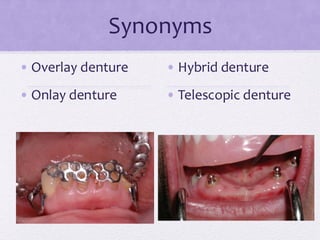
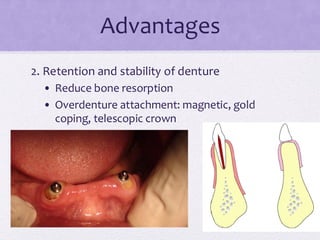
Advantages
2. Retention andstability of denture
• Reduce bone resorption
• Overdenture attachment: magnetic, gold
coping, telescopic crown
13.
Advantages
3. Improves occlusalstress distribution
Stress will be shared by the abutments and
edentulous ridge.
(Thayer & Caputo 1979)
4. Increased occlusal forces
• Improves masticatory performances and
chewing efficiency
Denture vs implant
overdenture
•Bite forces in mandibular implant retained
overdentures is higher than conventional
dentures.
(Fontjin-Tekamp et al 1998)
• Masticatory performance and chewing experience
in implant retained OD higher than conventional
dentures.
(Geertman et al 1999)
16.
Dentures vs
overdentures
• Biteforce & chewing efficiency:
• Natural tooth > Tooth supported overdenture >
implant supported overdenture > conventional
complete denture
(Fontjin-Tekamp et al 2000)
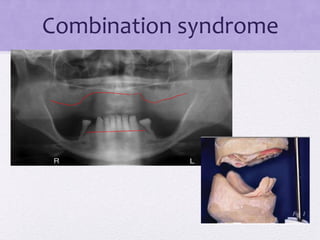
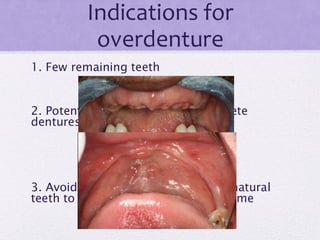
Combination syndrome
Complete maxillarydenture opposing partially
edentulous mandible with only anterior teeth remaining.
1. Loss of bone at anterior maxillary ridge
2. Enlarged maxillary tuberosities
3. Papillary hyperplasia at hard palate
4. Extrusion of lower anterior teeth
5. Loss of bone under the partial denture bases
(Kelly E., 1972)
Overlay denture onthe lower will utilize
the lower tooth roots for stabilization &
provide a complete denture occlusion.
(Kelly 1972)
Preservation of anterior maxillary teeth will
protect the ridge from resorption and
prevent Combination Syndrome.
(Langer & Langer 1992)
Advantages
8. Psychological advantagesfor patients
• Positive perception regarding a retained natural
feeling.
“I still have some of my own teeth to hold my
denture”
24.
Advantages: Conclusion
Maintain teethas part of the residual
ridge
1. Increase support
2. Able to withstand more occlusal
load
3. Improve retention
4. Psychological
Reduce the rate of bone resorption Alveolar bone to support the teeth
Retaining propriception Increase patients’ manipulative skills
to handle dentures
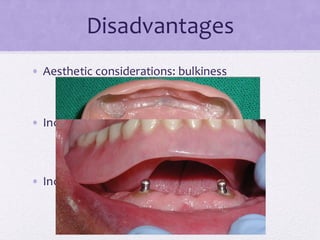
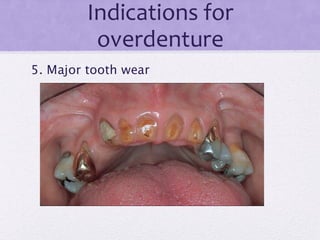
Disadvantages
• Limitation ofspace due to wear or
compensatory growth
• Potential for fracture of denture base
materials
• Risk of further disease of abutment: caries,
periodontal disease
Selection of abutment
teeth
1.Periodontal and mobility status
❑ Healthy periodontal tissues
❑ Rendered healthy by periodontal treatment
❑ Circumferential band of attached gingival
around abutment
❑ Mobility of not more than Grade II
35.
Selection of abutment
teeth
2.Abutment location
❑ The best: canines and premolars
❑ Upper anterior incisors, if mandibular teeth
still present.
❑ At least one tooth per quadrant
❑ The abutments must not be adjacent (if more
than one abutment)
36.
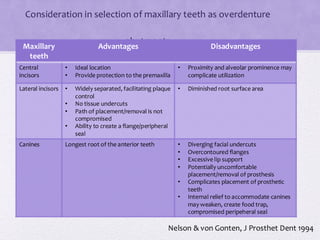
Consideration in selectionof maxillary teeth as overdenture
abutments
Maxillary
teeth
Advantages Disadvantages
Central
incisors
• Ideal location
• Provide protection to the premaxilla
• Proximity and alveolar prominence may
complicate utilization
Lateral incisors • Widely separated, facilitating plaque
control
• No tissue undercuts
• Path of placement/removal is not
compromised
• Ability to create a flange/peripheral
seal
• Diminished root surface area
Canines Longest root of the anterior teeth • Diverging facial undercuts
• Overcontoured flanges
• Excessive lip support
• Potentially uncomfortable
placement/removal of prosthesis
• Complicates placement of prosthetic
teeth
• Internal relief to accommodate canines
may weaken, create food trap,
compromised peripeheral seal
Nelson & von Gonten, J Prosthet Dent 1994
37.
Selection of abutment
teeth
3.Endodontic and Prosthodontic status
❑Anterior single rooted teeth are easier and less
expensive.
❑If pulpal recession to the extend of calcification
occurred, endodontic treatment can be
avoided.
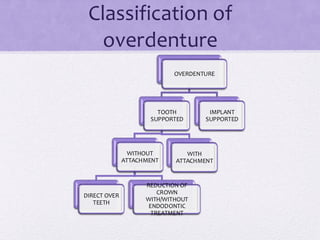
Overdentures: the
principles
• ToRCT or not?
• RCT increases the coronal reduction that can be
achieved.
• Elderly patient: sclerosed canals
• Severe toothwear: to RCT or not?
11% (52 out of 448) of tooth wear cases need RCT
(Sivasithamparam et al 2003)
40.
Overdentures: the
principles
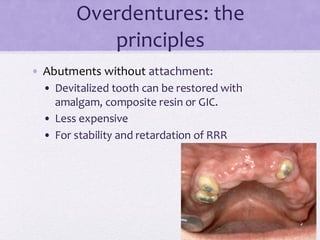
• Abutmentswithout attachment:
• Devitalized tooth can be restored with
amalgam, composite resin or GIC.
• Less expensive
• For stability and retardation of RRR
41.
Overdentures: the
principles
• Abutmentswith attachment mechanism on
cast coping:
• intracoronal/extracoronal attachments.
• Provide prosthesis retention.
• Disadvantages:
• Interarch space
• Increase costs
• Technique sensitive
• Demanding oral hygiene maintenance
Clinical procedures
• Toothsupported immediate complete
dentures
• Prepare the dentures and complete endodontic
treatment.
• Reduction of coronal portion of abutment teeth
prior to insertion of dentures
Clinical procedures
• Toothsupported overdenture with attachment
• Prepare the dentures and complete endodontic
treatment.
• Reduction of coronal portion of abutment
teeth.
• Cementation of attachment to the abutment
teeth
• Impression followed by construction of
dentures.
Loss of abutmentteeth
• The most frequent causes of abutment loss:
• Caries
• Periodontal disease
• Endodontic complications
• Poor clinical follow-up and patient compliance.
51.
Gingival irritation of
abutmentteeth
• The causes:
• Movement of denture base (esp mandibular
denture)
• Poor oral hygiene
• “dead space”: source of inflammation and
tissue hypertrophy and hyperplastic response.
52.
Loss of overdentureabutments was only 4.2%.
Mostly due to caries and periodontal diseases.
(Ettinger 1988)
Possible to maintain teeth as overdenture
abutments with good oral hygiene.
(Budtz- Jorgensen 1995)
53.
81% of three-teethtelescopic overdentures were
maintained at 8 years.
But…
Loss of dentures were more of a problem than
loss of abutments!
(Griess, Reilmann and Chanavaz 1998)
54.
• Tooth andtissue supported overdenture vs
tooth supported overdenture
• Abutment failure rate are the same.
• Abutment present: 84% at 5 years and 66% at 10
years.
(Wenz et al 2001)
Overdentures:
maintenance
• Abutments areexamined every 6-monthly
• Patient is instructed to brush over
abutments twice daily.
• Dentures must be kept clean.
• Chlorhexidine mouthwash
• Topical fluoride 1x/day using denture as
applicator.
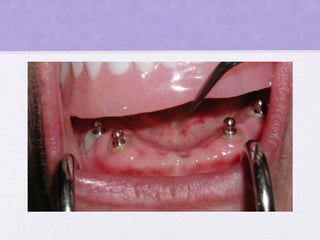
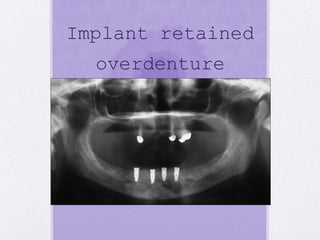
Implant retained
overdenture
• Dentureswhich utilize dental implants for
retention and support.
• Superior retention and stability
• Reduce the amount of soft tissue coverage
Patients with implantsupported
overdenture has significantly higher
quality of life than patients with
conventional dentures.
Mc Gill Consensus Statement 2002
Implant supported overdenture is the
standard of care to edentulous patients.
61.
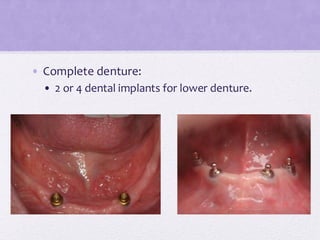
York Consensus Statement(2009)
Mandibular 2 implant-supported
overdenture is the first choice
standard of care for edentulous
patients.
62.
Less bone resorption
70%implant supported overdenture patients has
bone resorption of less than 0.2mm during the
first year and 0.6 mm in 5 years.
(Schwartz-Arad et al)
63.
Greater prosthesis
stability
• Implantretained overdenture is more stable.
• Conventional mandibular denture moves
during function:
• Soft tissue abrasion
• Accelerate bone loss
• Clicking noise during speech
64.
Indications for implant
overdentures
•Patients who lose their teeth in advanced age.
• Poor control of the dentures:
• Patient who had complete dentures for many years,
but lose their motor skills and no longer feel able to
wear complete dentures.
• This problem is observed much more often for the
edentulous mandible than maxilla.
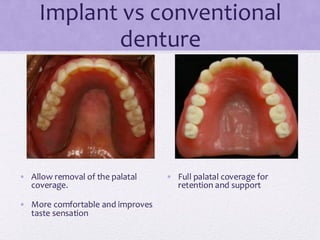
Implant vs conventional
denture
•Allow removal of the palatal
coverage.
• More comfortable and improves
taste sensation
• Full palatal coverage for
retention and support