Downloaded 265 times




































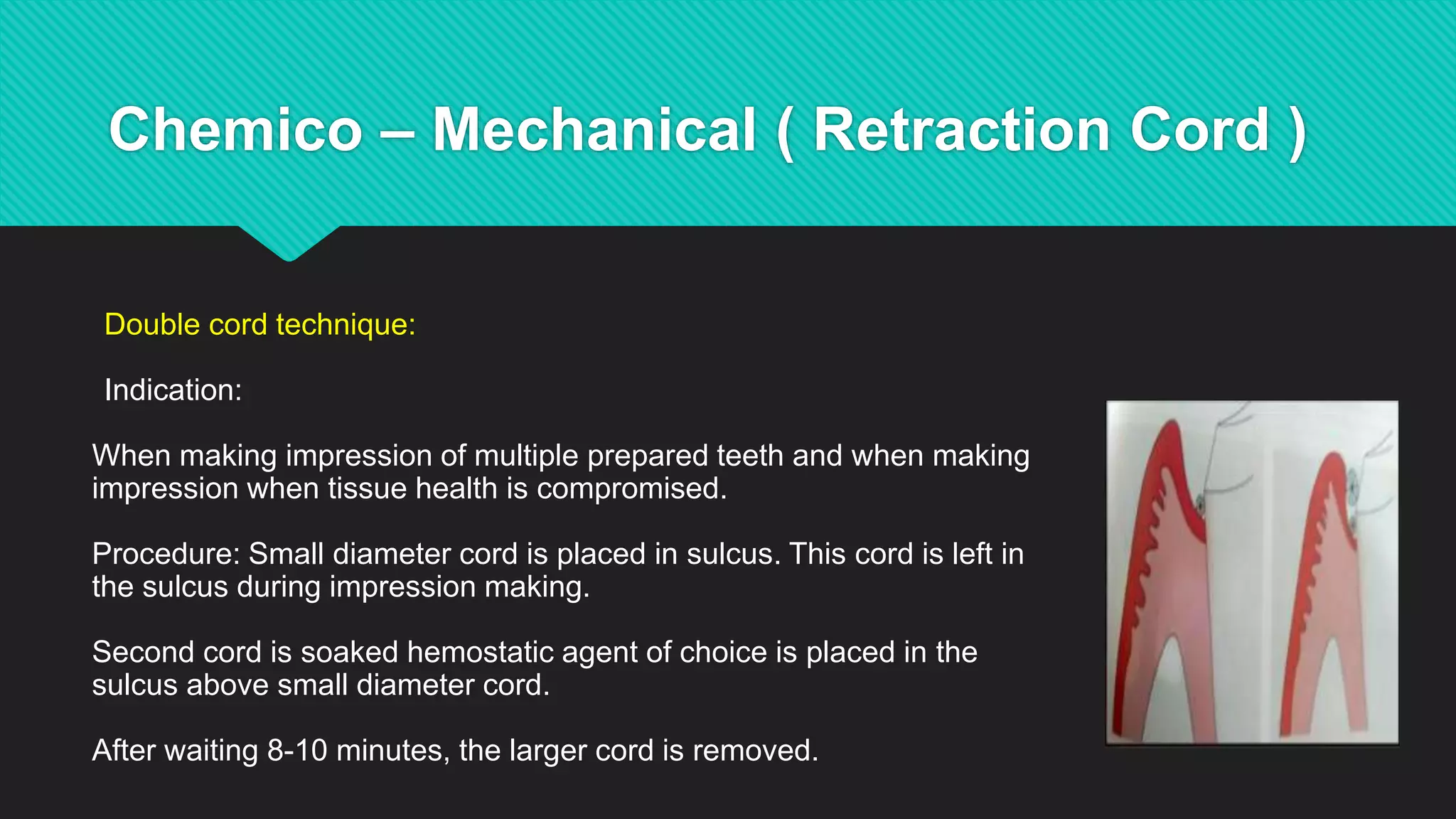


































The double cord technique involves placing a small diameter cord in the gingival sulcus first, leaving it in place, and then packing a larger diameter cord over the first cord to provide additional retraction and hemostasis for making impressions of multiple prepared teeth or when the gingival tissues are compromised. The small inner cord provides retraction while the outer cord provides additional hemostasis and tissue displacement needed for accurate impressions.



































































