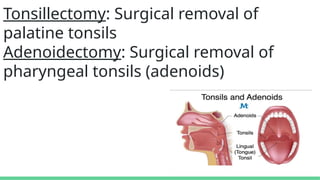
INDICATIONS: TONSILLECTOMY
A. ABSOLUTE
1.Recurrent infections of throat (most common)
(a) Seven or more episodes in 1 year, or
(b) Five episodes per year for 2 years, or
(c) Three episodes per year for 3 years, or
(d) Two weeks or more of lost school or work in 1 year.
2. Peritonsillar abscess.
3. Tonsillitis which causes febrile seizures.
5.
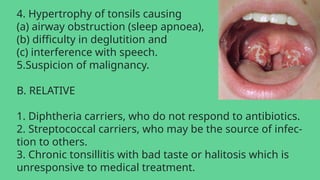
4. Hypertrophy oftonsils causing
(a) airway obstruction (sleep apnoea),
(b) difficulty in deglutition and
(c) interference with speech.
5.Suspicion of malignancy.
B. RELATIVE
1. Diphtheria carriers, who do not respond to antibiotics.
2. Streptococcal carriers, who may be the source of infec-
tion to others.
3. Chronic tonsillitis with bad taste or halitosis which is
unresponsive to medical treatment.
6.
4. Recurrent streptococcaltonsillitis in a patient with val-
vular heart disease.
C. AS A PART OF ANOTHER OPERATION
1. Palatopharyngoplasty which is done for sleep apnoea
syndrome.
2. Glossopharyngeal neurectomy. Tonsil is removed first
and then IX nerve is severed in the bed of tonsil.
3. Removal of styloid process.
7.
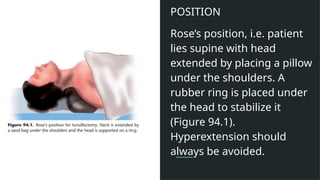
POSITION
Rose’s position, i.e.patient
lies supine with head
extended by placing a pillow
under the shoulders. A
rubber ring is placed under
the head to stabilize it
(Figure 94.1).
Hyperextension should
always be avoided.
8.
STEPS OF OPERATION(DISSECTION
AND SNARE METHOD)
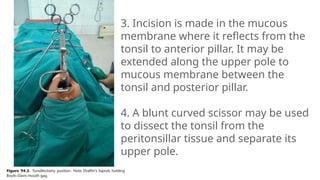
1. Boyle–Davis mouth gag is introduced and opened. It is
held in place by Draffin’s bipods or a string over a pulley.
2. Tonsil is grasped with tonsil-holding forceps and
pulled medially.
9.
3. Incision ismade in the mucous
membrane where it reflects from the
tonsil to anterior pillar. It may be
extended along the upper pole to
mucous membrane between the
tonsil and posterior pillar.
4. A blunt curved scissor may be used
to dissect the tonsil from the
peritonsillar tissue and separate its
upper pole.
11.
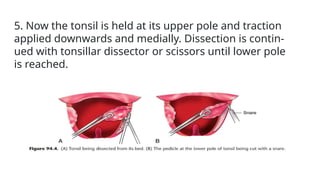
5. Now thetonsil is held at its upper pole and traction
applied downwards and medially. Dissection is contin-
ued with tonsillar dissector or scissors until lower pole
is reached.
12.
6. Now wireloop of tonsillar snare is threaded over the
tonsil on to its pedicle, tightened, and the pedicle cut
and the tonsil removed.
7. A gauze sponge is placed in the fossa and pressure ap-
plied for a few minutes.
8. Bleeding points are tied with silk. Procedure is repeated
on the other side.
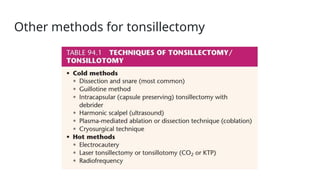
Guillotine method -Largely abandoned. It can be done only
when tonsils are mobile and tonsil bed has not been scarred
by repeated infections.
Intracapsular tonsillectomy - With the use of powered
instrument (debrider) tonsil is removed but its capsule is
preserved in the hope to reduce postoperative pain.
Harmonic scalpel - It uses ultrasound to cut and coagulate
tissues. causes less tissue damage and less postoperative
pain compared to electrocautery technique.
Plasma-mediated ablation technique - In this ablation
method, protons are energized to break molecular bonds
between tissues.
15.
Cryosurgical technique -Tonsil is frozen by application of
cryoprobe and then allowed to thaw. Two applications, each of
3–4 min, are applied. Tonsillar tissue will undergo necrosis and
later fall off leaving a granulating surface.
Electrocautery - Both unipolar and bipolar electrocautery has
been used. It reduces blood loss but causes thermal injury to
tissues.
Laser tonsillotomy - which aims to reduce the size of tonsils.
It is indicated in patients who are unable to tolerate general
anaesthesia.
16.
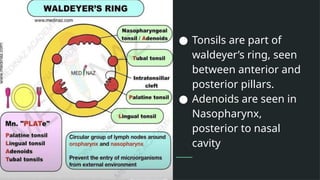
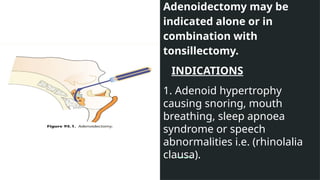
Adenoidectomy may be
indicatedalone or in
combination with
tonsillectomy.
INDICATIONS
1. Adenoid hypertrophy
causing snoring, mouth
breathing, sleep apnoea
syndrome or speech
abnormalities i.e. (rhinolalia
clausa).
17.
2. Recurrent rhinosinusitis.
3.Chronic otitis media with
effusion associated with
adenoid hyperplasia.
4. Recurrent ear discharge
in benign CSOM associated
with adenoiditis/adenoid
hyperplasia.
5. Dental malocclusion.
Adenoidectomy does not
correct dental
abnormalities
35
22
but will prevent its
recurrence after
orthodontic treatment.
POSITION
Same as for tonsillectomy.
Hyperextension of neck
should always be avoided
18.
STEPS OF OPERATION
1.Boyle–Davis mouth gag is inserted. Before actual
removal of adenoids, nasopharynx should always be
examined by retracting the soft palate with curved end of
the tongue depressor and by digital palpation, to confirm
the diagnosis, to assess the size of adenoids mass and to
push the lateral adenoid masses towards the midline. A
laryngeal mirror helps to assess the size and extent of
adenoid mass
19.
2. Proper sizeof “adenoid curette with guard” is introduced
into the nasopharynx till its free edge touches the
posterior border of nasal septum and is then pressed
backwards to engage the adenoids.
At this level, head should be slightly flexed to avoid injury
to the odontoid process.
3. With gentle sweeping movement, adenoids are shaved
off Lateral masses are similarly removed with smaller
curettes; small tags of lymphoid tissue left behind are
removed with punch forceps.
Take care not to injure pharyngeal ends of eustachian
tubes.
20.
4. Haemostasis isachieved by packing the area for some
time. Persistent bleeders are electrocoagulated under
vision. If bleeding is still not controlled, a postnasal pack is
left for 24 h.
ENDOSCOPIC ADENOIDECTOMY
These days adenoids can be removed more precisely by
using a debrider under endoscopic control or by coblation
technique.