Thyroid & antithyroid drugs
•Download as PPT, PDF•
40 likes•1,754 views

This document summarizes thyroid hormone synthesis and regulation. It discusses that the thyroid gland secretes three hormones: thyroxine (T4), triiodothyronine (T3), and calcitonin. T4 and T3 are synthesized through a process involving iodine uptake, oxidation, iodination of tyrosine residues, and coupling reactions. T4 has lower activity than T3, which is produced from peripheral conversion of T4. The hormones act through nuclear receptors to increase metabolism. The document also outlines treatments for hyperthyroidism including antithyroid drugs, iodine, beta blockers, and radioactive iodine, which destroy the thyroid tissue.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Thyroid & antithyroid drugs
Similar to Thyroid & antithyroid drugs (20)
More from BikashAdhikari26
More from BikashAdhikari26 (20)
Recently uploaded
Recently uploaded (20)
Thyroid & antithyroid drugs
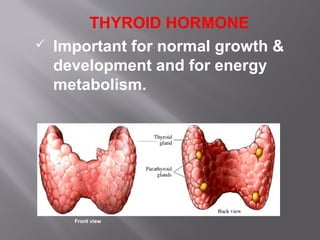
- 1. THYROID HORMONE Important for normal growth & development and for energy metabolism. Front view
- 2. THYROID HORMONE Thyroid Gland secretes 3 hormones Thyroxine (T4) Triiodothyronin (T3) – Thyroid hormones - produced by follicles Calcitonin – produced by interfollicular ‘C’ cells
- 3. RELEASE
- 4. SYNTHESIS AND RELEASE OF HORMONE I. Uptake of plasma iodide by the follicle cells (Iodide trapping) II. Oxidation of iodide and iodination of tyrosine (Oxidation & iodination) III. Coupling IV. Storage and release V. Peripheral Conversion of T4 to T3
- 5. I. IODINE TRAPPING: Energy dependent process against a gradient (Na+ /I- symport; NIS) Trapping is also present in other gland but not stimulated by TSH II. OXIDATION & IODINATION: I- to I+ with the help of H2O2 & catalysed by peroxidase enzyme I+ combine with tyrosine to form MIT and DIT
- 6. III. COUPLING: MIT and DIT couple together to form T3 and T4 Peroxidase enzyme catalyse Takes place in and facilitated by Thyroglobulin (TG) IV. STORAGE AND RELEASE: These thyroglobulin remains stored as thyroid colloid in the interior of follicles Taken into cell by endocytosis; lysosomal protease breaks down T3, T4 is secreted & MIT, DIT are deiodinated and utilised
- 7. Coupling Reactions DIT+DIT=T4 MIT+DIT=T3 Coupling Reactions MIT+DIT=T3 DIT+DIT=T4 Thyroid Hormone Synthesis NIS-Sodium Iodide Symporter, TPO-thyroid peroxidase
- 8. V. PERIPHERAL CONVERSION OF T4 TO T3: T3 (low concentration) is an active form Liver & kidney convert T4 to T3 Inhibitor - Propyl thiouracil, propranolol (highdose), amiodarone and glucocorticoids
- 9. TRANSPORTATION, METABOLISM & EXCRETION: Highly plasma protein bound Thyroxine binding protein (TBG), Thyroxine binding prealbumin, Albumin Metabolised by deiodination and conjugation in liver (kidney & salivary gland) Metabolite undergo enterohepatic circulation t1/2 of T4 = 6-7 days: t1/2 of T3 = 1-2 days
- 10. MOA: Both T3 and T4 penetrates cells by active transport & binds to nuclear thyroid hormone receptor bound to the thyroid hormone response element (TRE) Conformation changes occur (heterodimerization of receptor with retinoid X receptor (RXR)) & releases coreporessor and binding of coactivator occurs Gene transcription induced production of specific mRNA and proteins Metabolic and anatomic effects.
- 12. ACTIONS Affect whole body Growth and development: Essential for normal growth & development Congenital deficiency- milestones of development are delayed (mental retardation) Metabolism ↑ BMR Lipolysis - ↑ free fatty acid, LDL level ↓ Carbohydrate- ↑ peripheral utilization, glycogenolysis, gluconeogenesis & absorption - hyperglycemia Protein- Catabolism
- 13. CVS: ↑ Sensitivity & number of beta receptor - ↑HR, contractility and CO Skeletal muscle: Hypothyroidism- flabby and weak Hyperthyroidism- ↑ muscle tone, tremor, weakness GIT: Propulsive activity ↑es with hormones Haemopoiesis: Hypothyroidism- anaemia Reproduction: Hypothyroidism- impaired fertility Preparations: l-thyroxine sod. 25, 50, 75, 100 mcg- T4 (commonly used)
- 14. USES: 1. Cretinism: 2. Adult hypothyroidism: Symptoms ↓T3 & T4 and ↑TSH Levothyroxine - in empty stomach 50 mcg ODX 3wks then 100mcg OD for 3 wks----- Davidson’ medicine ↓Weight & periorbital puffiness in 2-3weeks Subclinical Hypothyroidism 3. Myxoedema coma: 4. Nontoxic goiter:
- 15. Thyroid inhibitor- reduce thyroid activity and hormonal effect Used in thyrotoxicosis Thyrotoxicosis means an excess of thyroid hormone in the body. Graves' disease is the major cause of hyperthyroidism. Other causes include multinodular goiter, toxic adenoma, inflammation of the thyroid & taking too much iodine. THYROID INHIBITORS
- 16. CLASSIFICATION 1. Hormone synthesis inhibitor (Antithyroid drugs): Propylthiouracil, Carbimazole, Methimazole 2. Ion trapping inhibitor: Thiocyanates, Perchlorates, Nitrates 3. Hormone release inhibitor: Iodine, Sod. and pot. Iodides 4. Destroy thyroid tissue: Radioactive iodine (131 I, 125 I, 123 I) PROLONG USE CAUSE HYPOTHYROIDISM: Lithium, Amiodarone, Sulfonamide, Phenytoin, Carbamazepine, rifampin, Phenobarbitone
- 17. ANTITHYROID DRUGS (Thioamides) MOA: Inhibit synthesis by binding to peroxidase enzyme & preventing its action Inhibit iodination of tyrosine residues in thyroglobulin Inhibit coupling of iodotyrosine residues to for T3 and T4 Thyroid colloid is depleted over time and blood levels of thyroid hormones are progressively lowered. Propylthiouracil (PTU), in addition, inhibit peripheral conversion of T4 to T3 Carbimazole (prodrug) converts to
- 18. Antithyroid drugs Contd……… Pharmacokinetics Quick oral absorption Concentrate in gland – large Vd Enter milk, cross placenta Metabolised in liver Adverse effects Reversible hypothyroidism & goiter on overtreatment GI intolerance, skin rashes & joint pain- important Loss or graying of hair, loss of taste, fever & liver damage- infrequent Reversible agranulocytosis- rare but serious
- 19. Antithyroid drugs Contd……… Propylthiouracil Carbimazole Less potent More potent High plasma proteinLess plasma protein bound bound Less excrete in milk More & less cross placenta Short t1/2 Long t1/2 Multiple dosing Single dosing No active metabolite Converts to methimazole (active) Inhibit peripheral No action conversion of T4- T3
- 20. USES: Thyrotoxicosis Grave’s Disease Toxic Nodular Goiter Make patient euthyroid before thyroidectomy Along with 131 I therapy
- 21. IODINE AND IODIDES: Fastest acting: initially cause “thyroid constipation” ; but after 10-15 days, “thyroid escape” MOA: Inhibition of hormone release- termed as ‘thyroid constipation’ Inhibits Endocytosis of colloid and proteolysis of thyroglobulin. Excess of iodine inhibits its own transport by interfering with expression of NIS Lugol’s iodine (5% iodine in 10 % potassium iodide solution)
- 22. USES (iodine & iodide): 1. Preoperative preparation: 10 days before thyroidectomy 2. Thyroid strom 3. Prophylaxis of endemic goiter 4. Antiseptic ADVERSE EFFECT (iodine & iodide): 1. Acute reaction: Sensitive person- swelling of lip & eyelids, fever, joint pain etc 2. Chronic overdose (iodism): Inflammation of mucous membranes, salivation, rhinorrhoea, sneezing, lacrymation, swelling of eyelids, burning sensation in mouth, headache, rashes, GI symptoms etc
- 23. RADIOACTIVE IODINE: 131 I - therapeutic value 125 I, 123 I - Diagnosis (rarely used) 131 I emits γ rays & β particles β radiation (cytotoxic action) penetrate 0.5- 2 mm only Dose - calculated in millicurie MOA: Given single dose orally as sod 131 I – concentrate in thyroglobulin→ β particles destroy thyroid parenchyma (few weeks)
- 24. β ADRENERGIC BLOCKER: Propranolol, Metoprolol, Atenolol etc (without intrensic sympathomimetic activity) – effective adjuvant Quick symptomatic relief (palpitation, tremor, nervousness, sweating, myopathy) without altering hormone level Propranolol (widely used) in high dose (160mg /day) reduce T3 level approx. 20% by inhibiting peripheral conversion Uses: Thyrotoxic crisis, while awaiting response to carbimazole or 131 I , preoperative preparation before surgery
Editor's Notes
- Signs of hypothyroidism: Dry skin, decreased sweating, thinning of the epidermis, and hyperkeratosis of the stratum corneum. Increased dermal glycosaminoglycan content traps water, giving rise to skin thickening without pitting (myxedema). Typical features include a puffy face with edematous eyelids and nonpitting pretibial edema. There is pallor, often with a yellow tinge to the skin due to carotene accumulation. Nail growth is retarded, and hair is dry, brittle, difficult to manage, and falls out easily. In addition to diffuse alopecia, there is thinning of the outer third of the eyebrows, although this is not a specific sign of hypothyroidism. Other common features include constipation and weight gain (despite a poor appetite). The weight gain is usually modest and due mainly to fluid retention in the myxedematous tissues. Libido is decreased in both sexes. Fertility is reduced and the incidence of miscarriage is increased. Myocardial contractility and pulse rate are reduced, leading to a reduced stroke volume and bradycardia. Blood flow is diverted from the skin, producing cool extremities. Fluid may also accumulate in other serous cavities and in the middle ear, giving rise to conductive deafness. Pulmonary function is generally normal, but dyspnea may be caused by pleural effusion, impaired respiratory muscle function, diminished ventilatory drive, or sleep apnea. Memory and concentration are impaired. Rare neurologic problems include reversible cerebellar ataxia, dementia, psychosis, and myxedema coma. The hoarse voice and occasionally clumsy speech of hypothyroidism reflect fluid accumulation in the vocal cords and tongue.