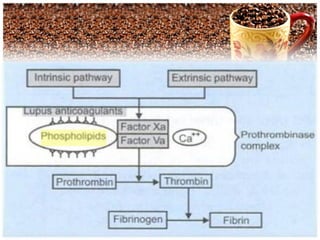
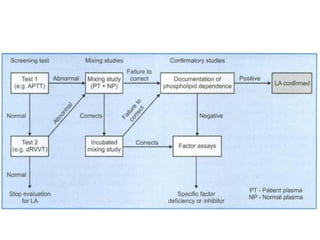
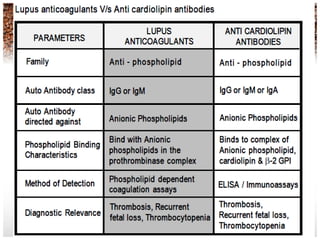



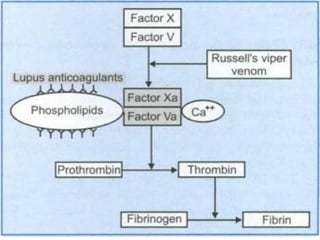



Lupus anticoagulants are autoantibodies that bind to phospholipids and prolong clotting tests that use phospholipids, such as APTT and DRVVT. They were first identified in 1952 in patients with systemic lupus erythematosus. While initially thought to cause bleeding, they are now known to be prothrombotic and associated with thrombosis. Their detection is important for diagnosis of antiphospholipid syndrome, which increases the risk of blood clots and pregnancy complications. The DRVVT test is most sensitive and specific for detecting lupus anticoagulants due to its use of varying phospholipid concentrations to demonstrate phospholipid dependence.























































































