Download as PDF, PPTX
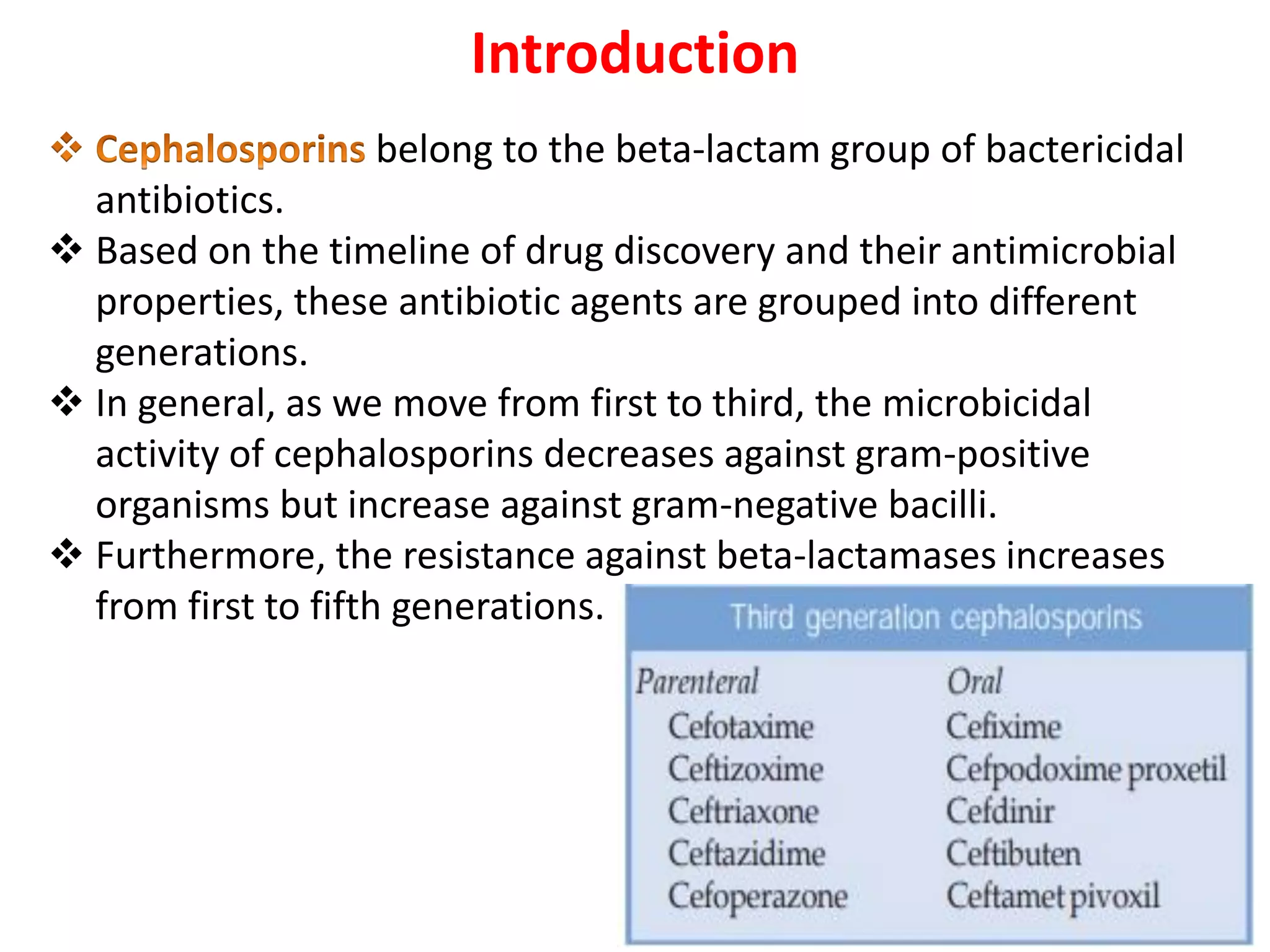
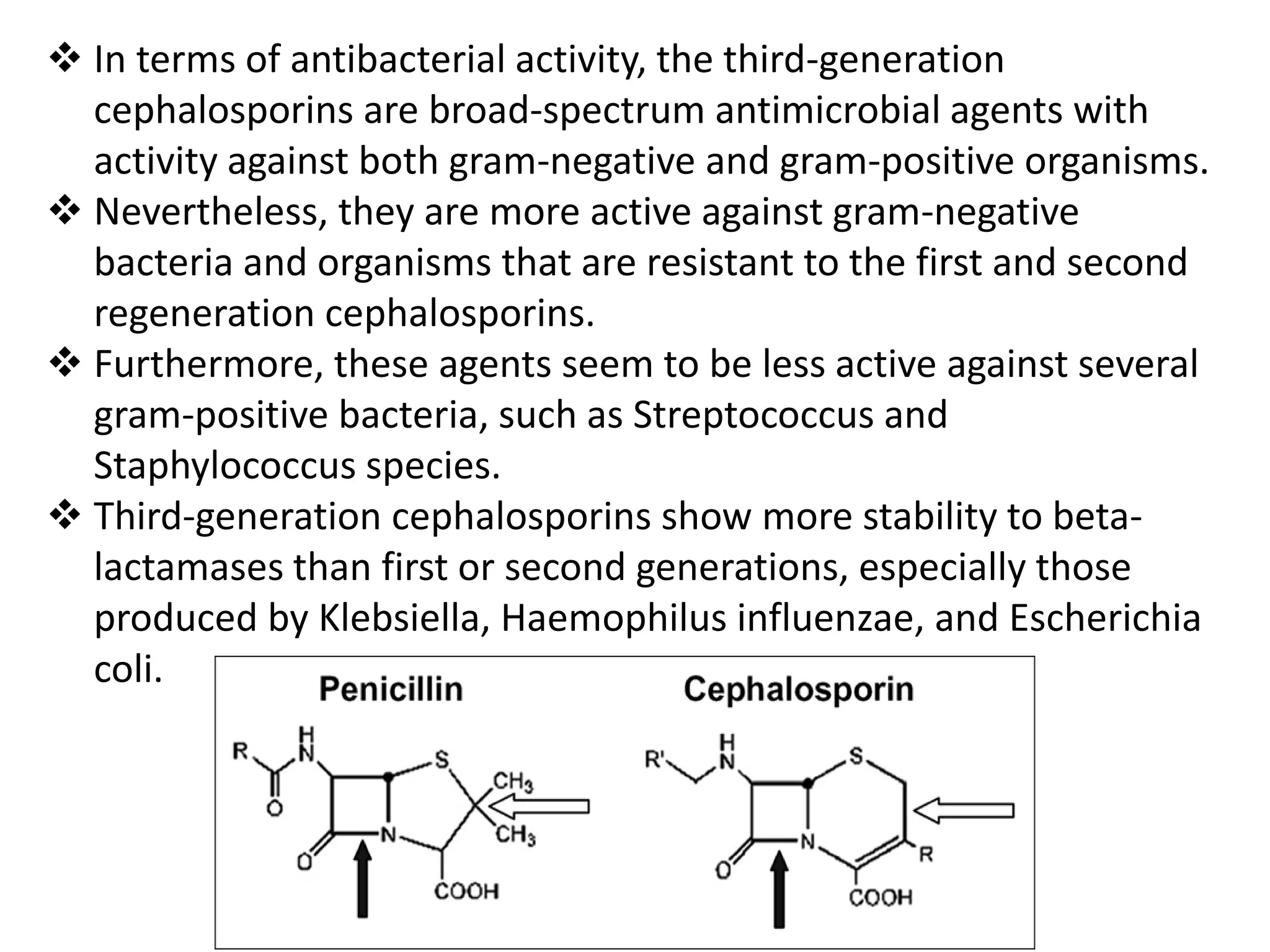
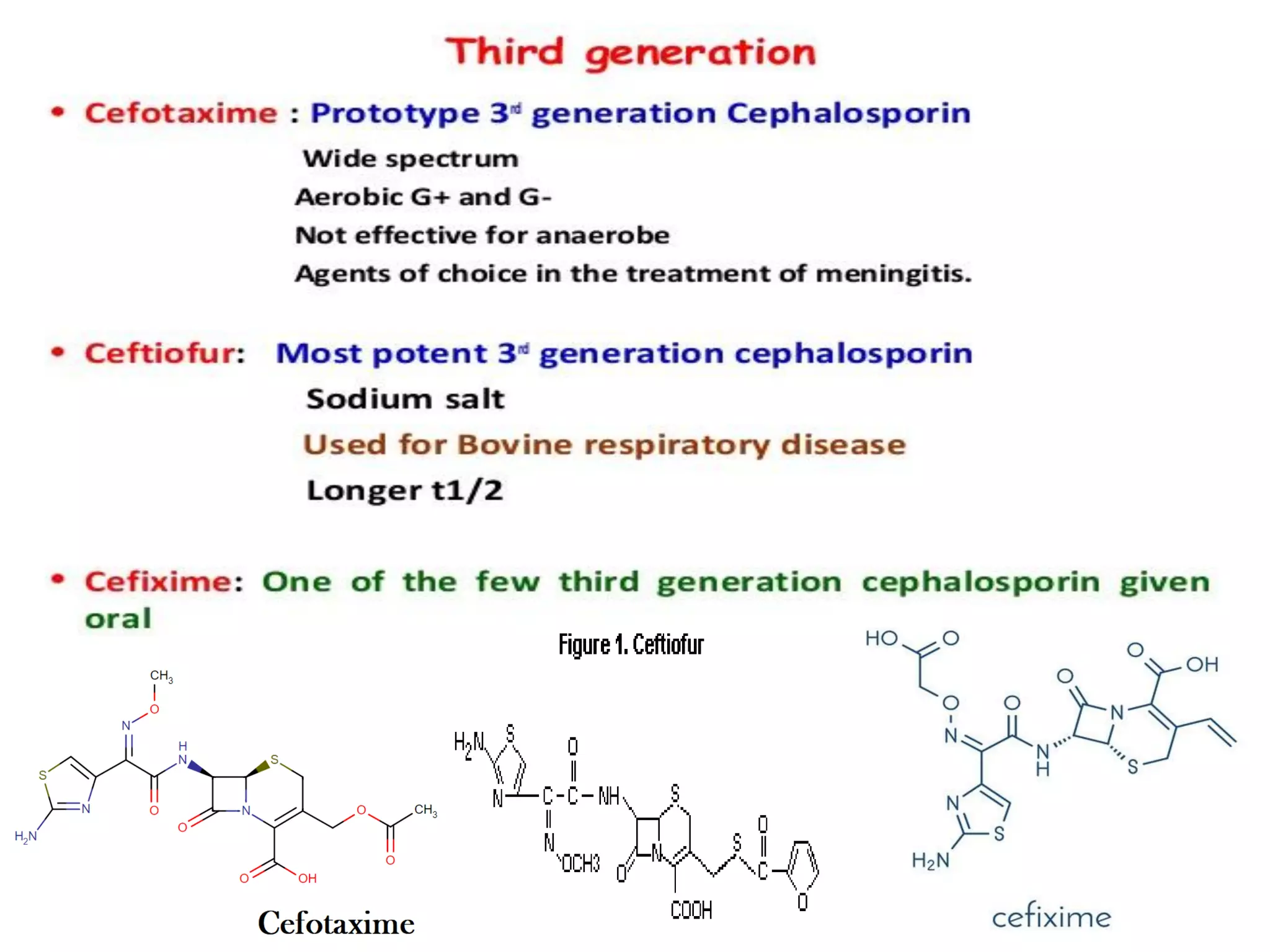
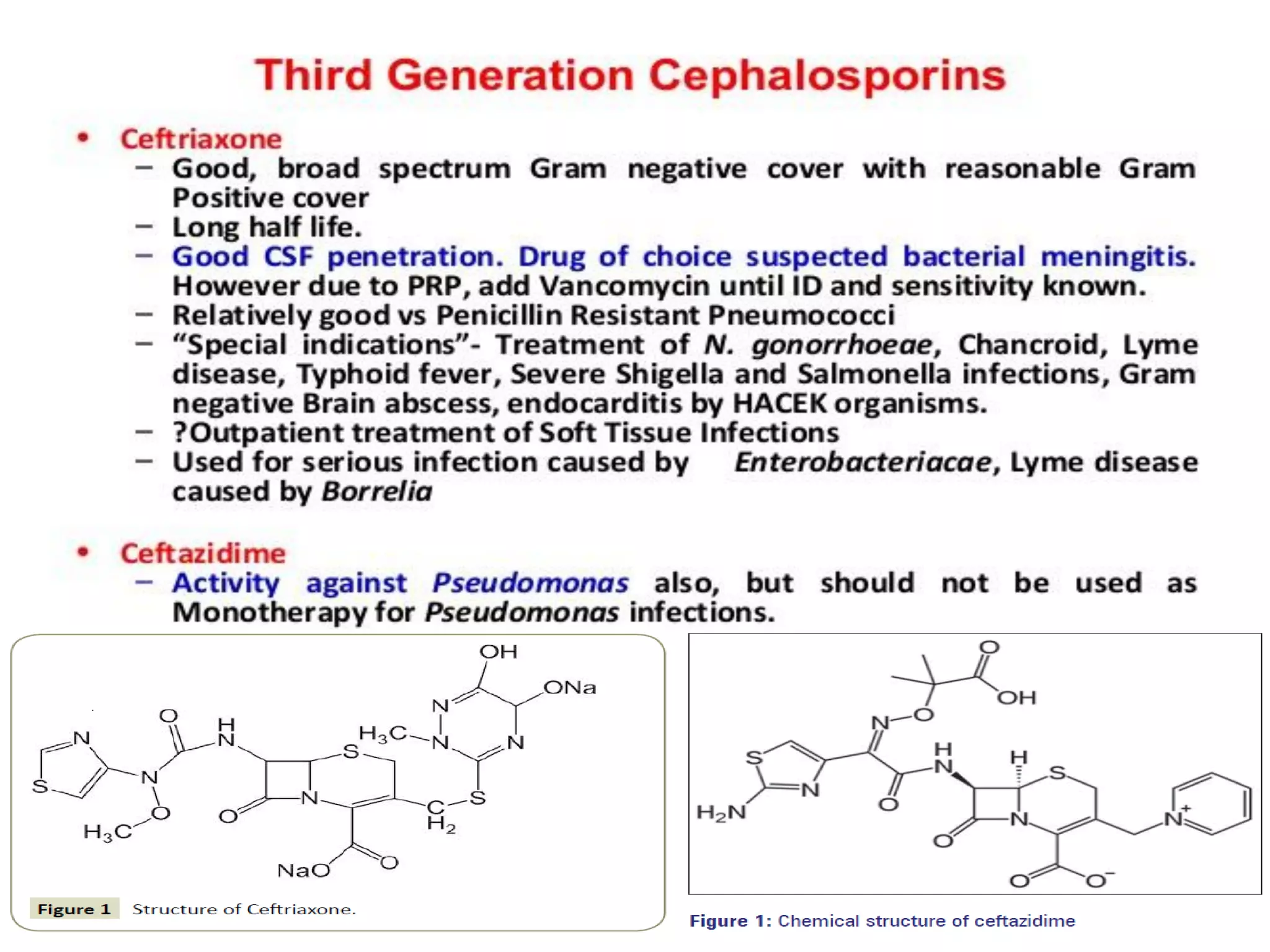
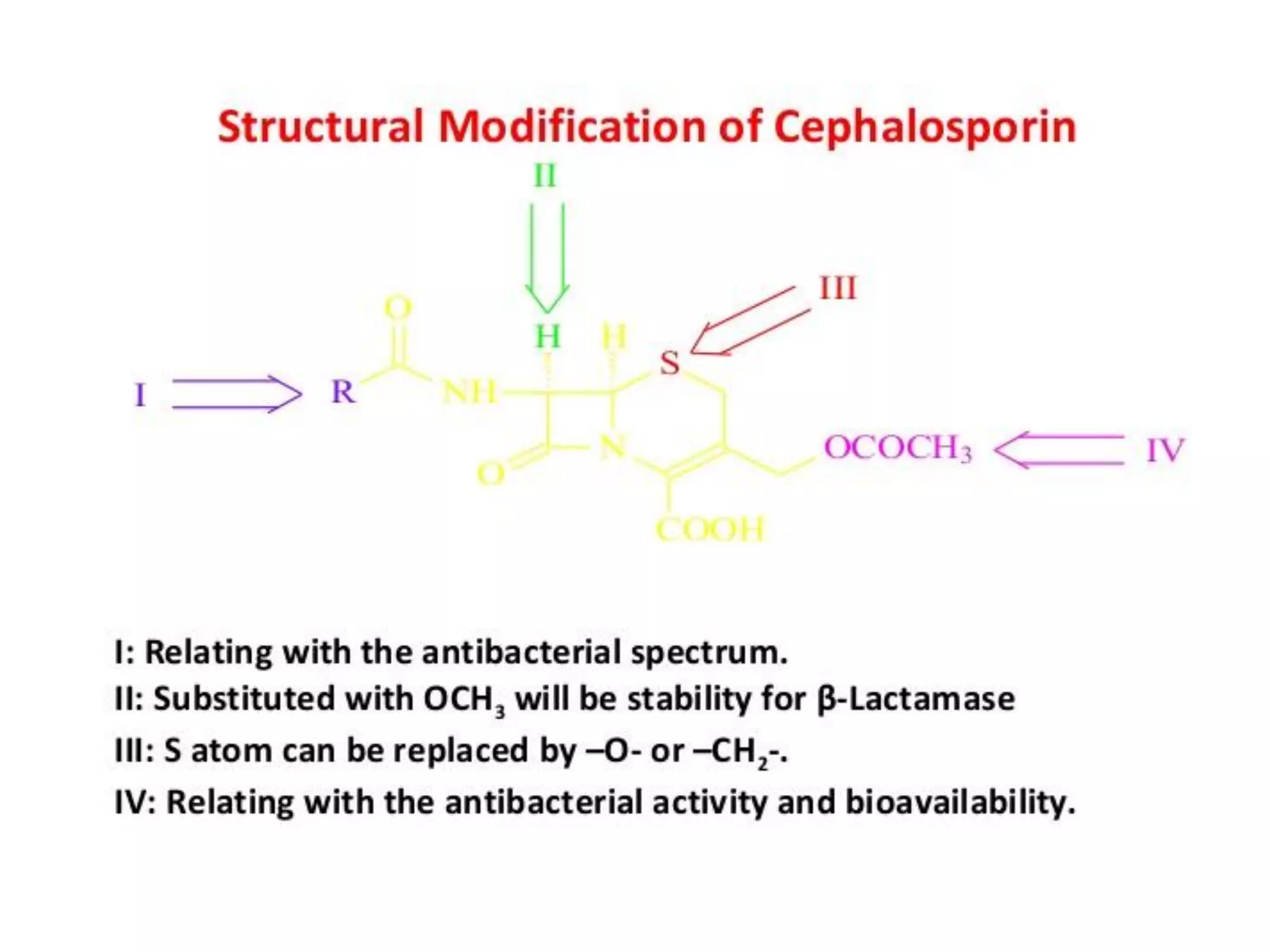
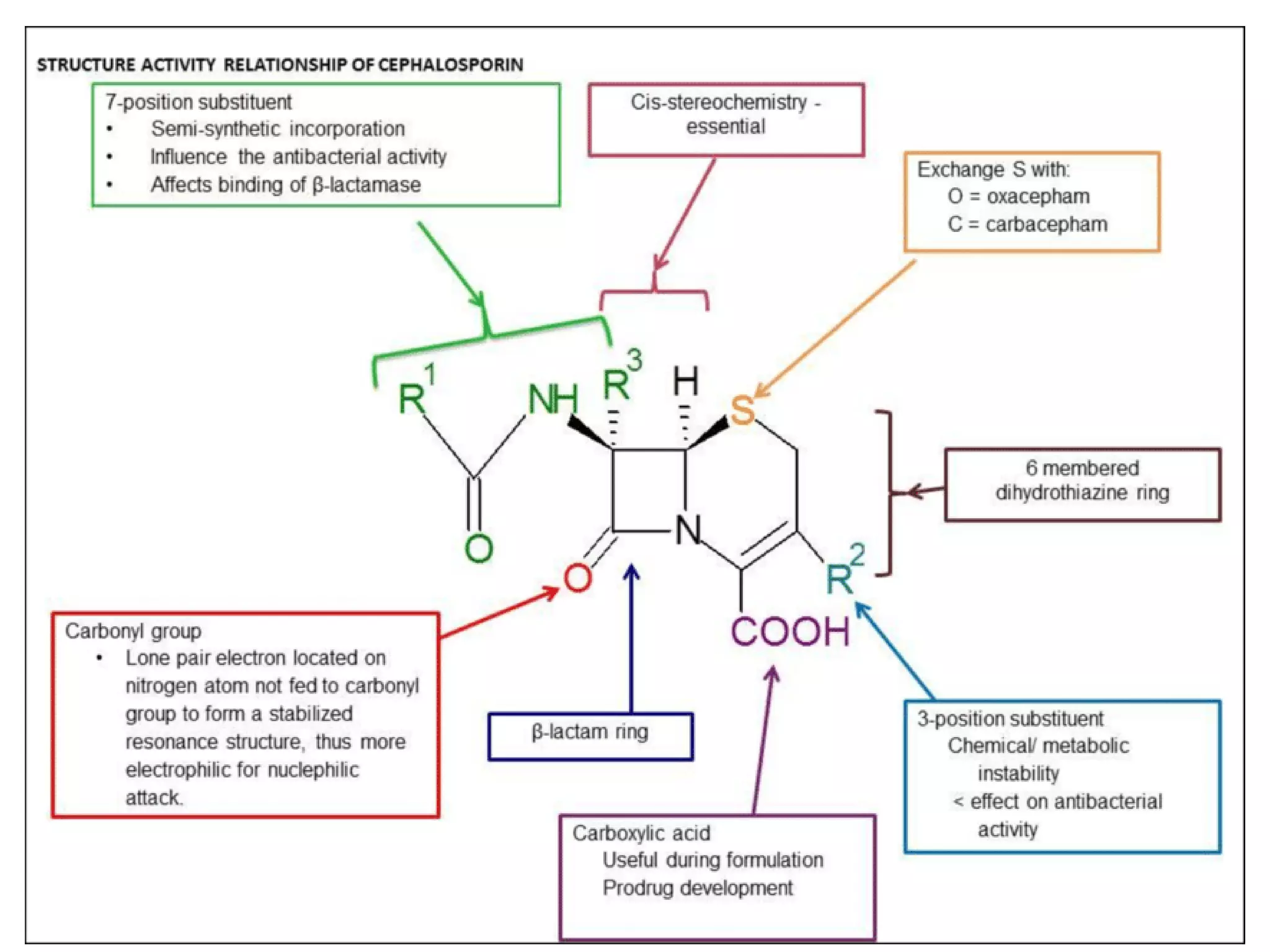
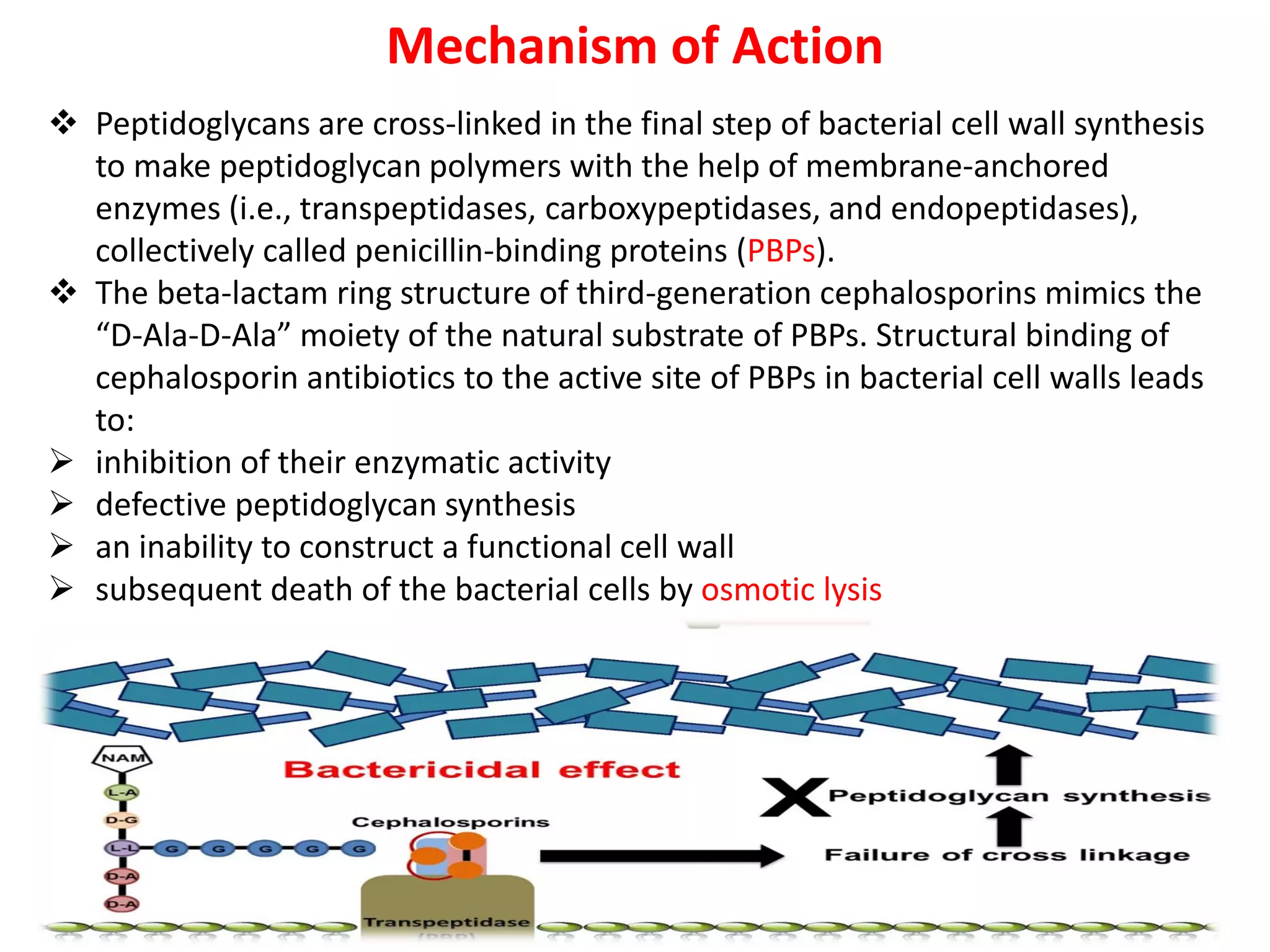



The document provides an overview of third-generation cephalosporins, highlighting their structure-activity relationship, pharmacokinetics, mechanism of action, clinical uses, adverse effects, and resistance issues. These antibiotics are primarily effective against gram-negative bacteria, showing increased stability to beta-lactamases and are often used in cases where other antibiotics are ineffective. While they are beneficial for various infections, there are still considerations regarding allergies, contraindications, and the emergence of resistant strains.



































































