Downloaded 162 times








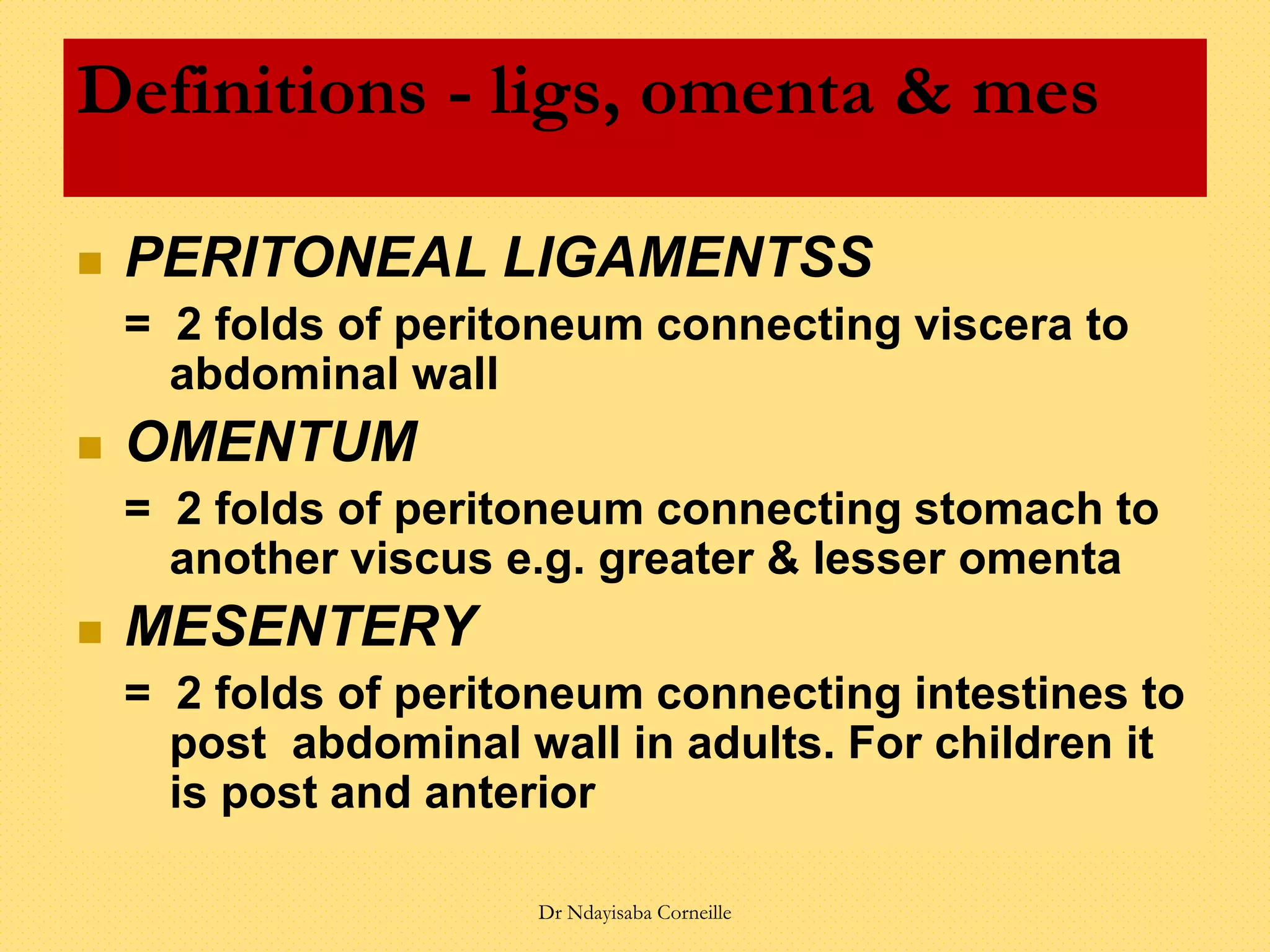




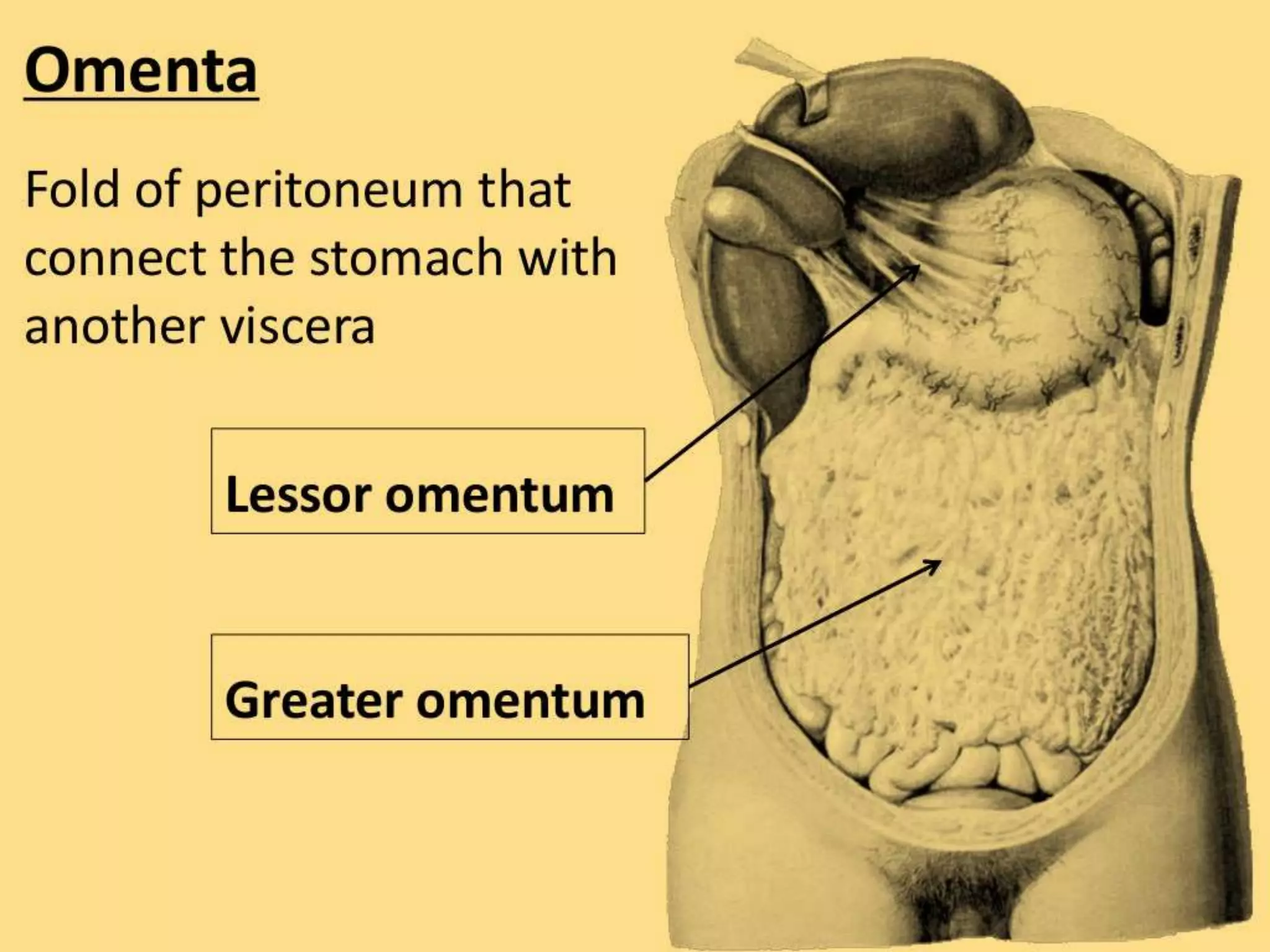



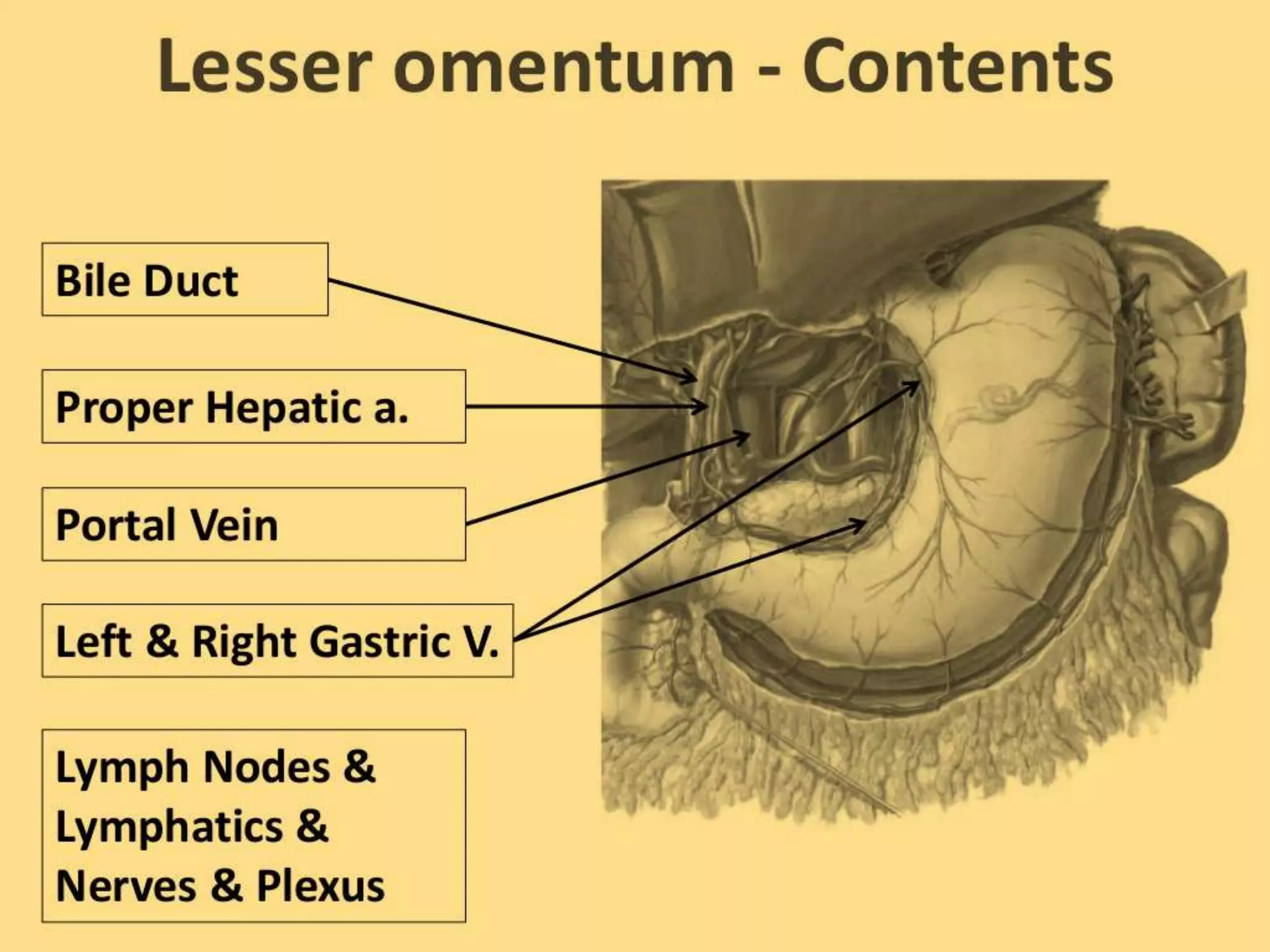

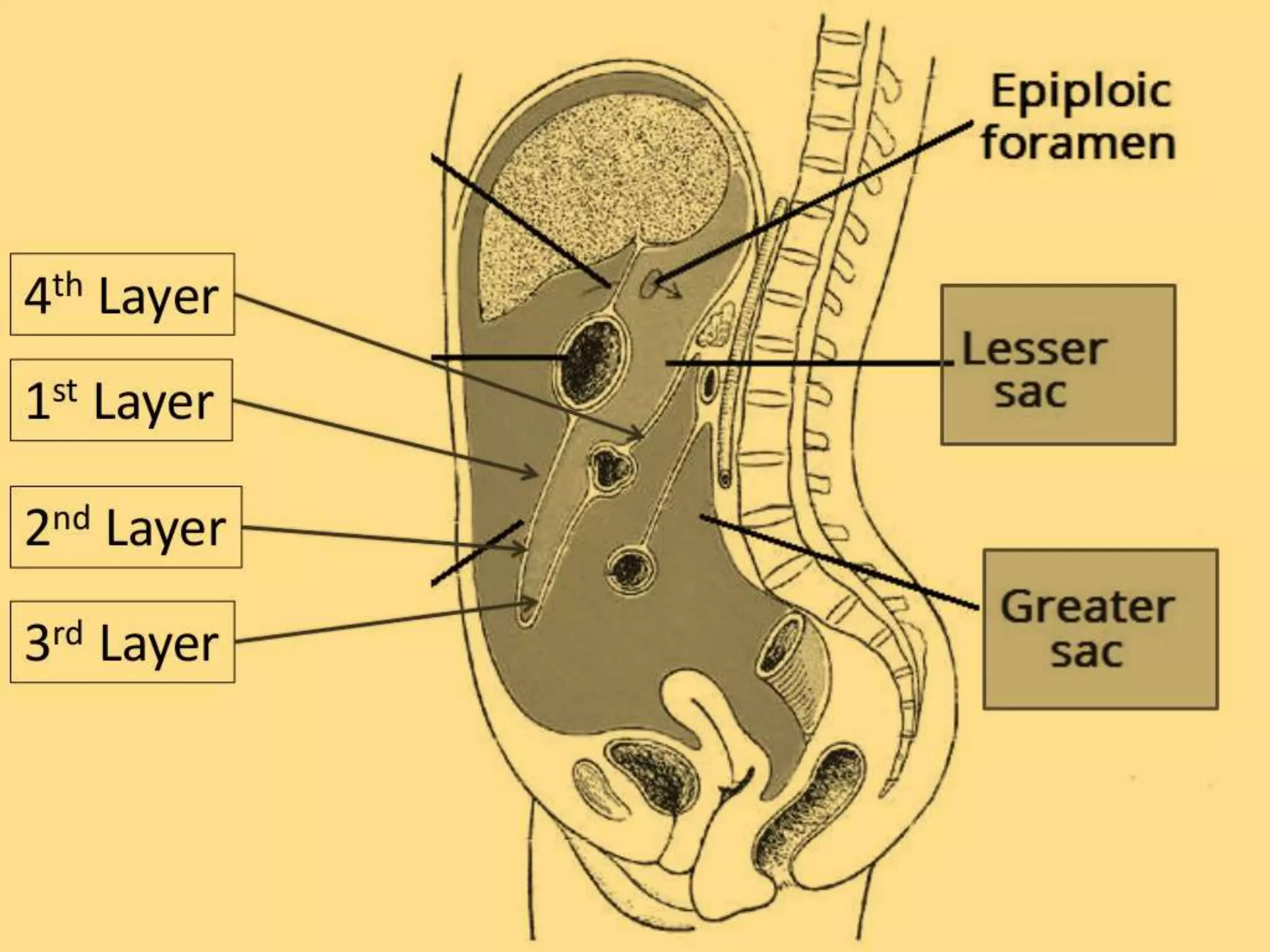

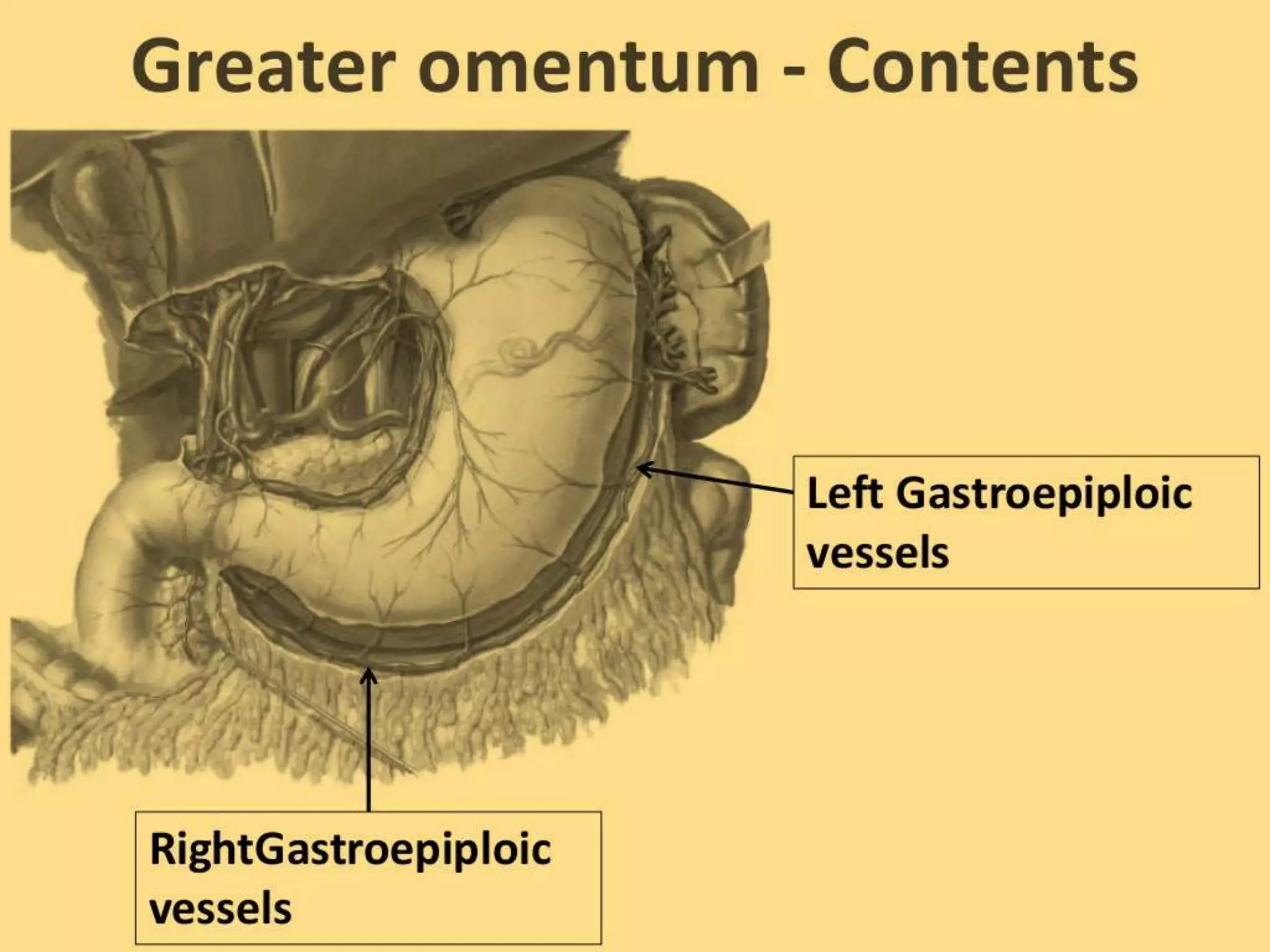




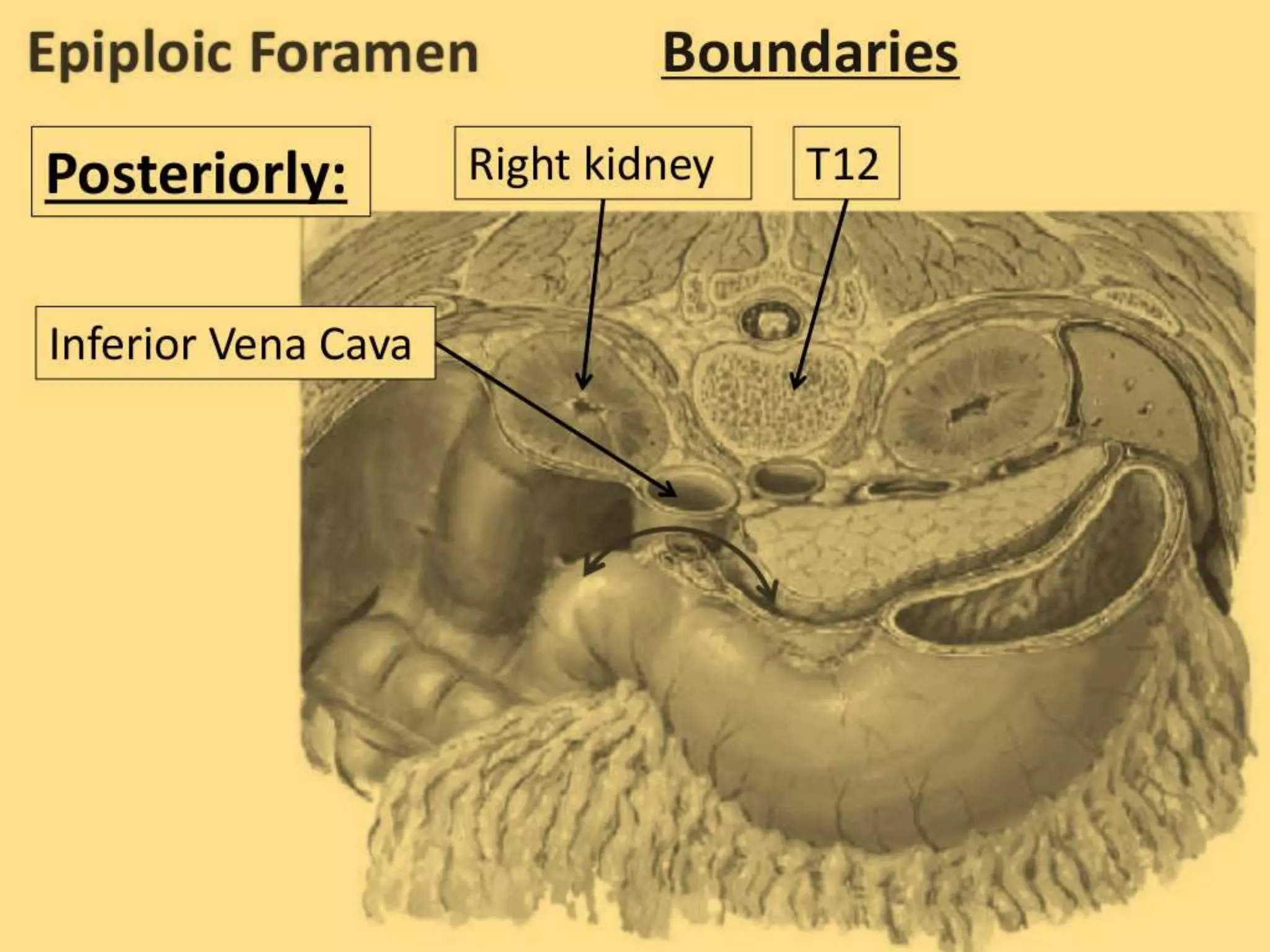
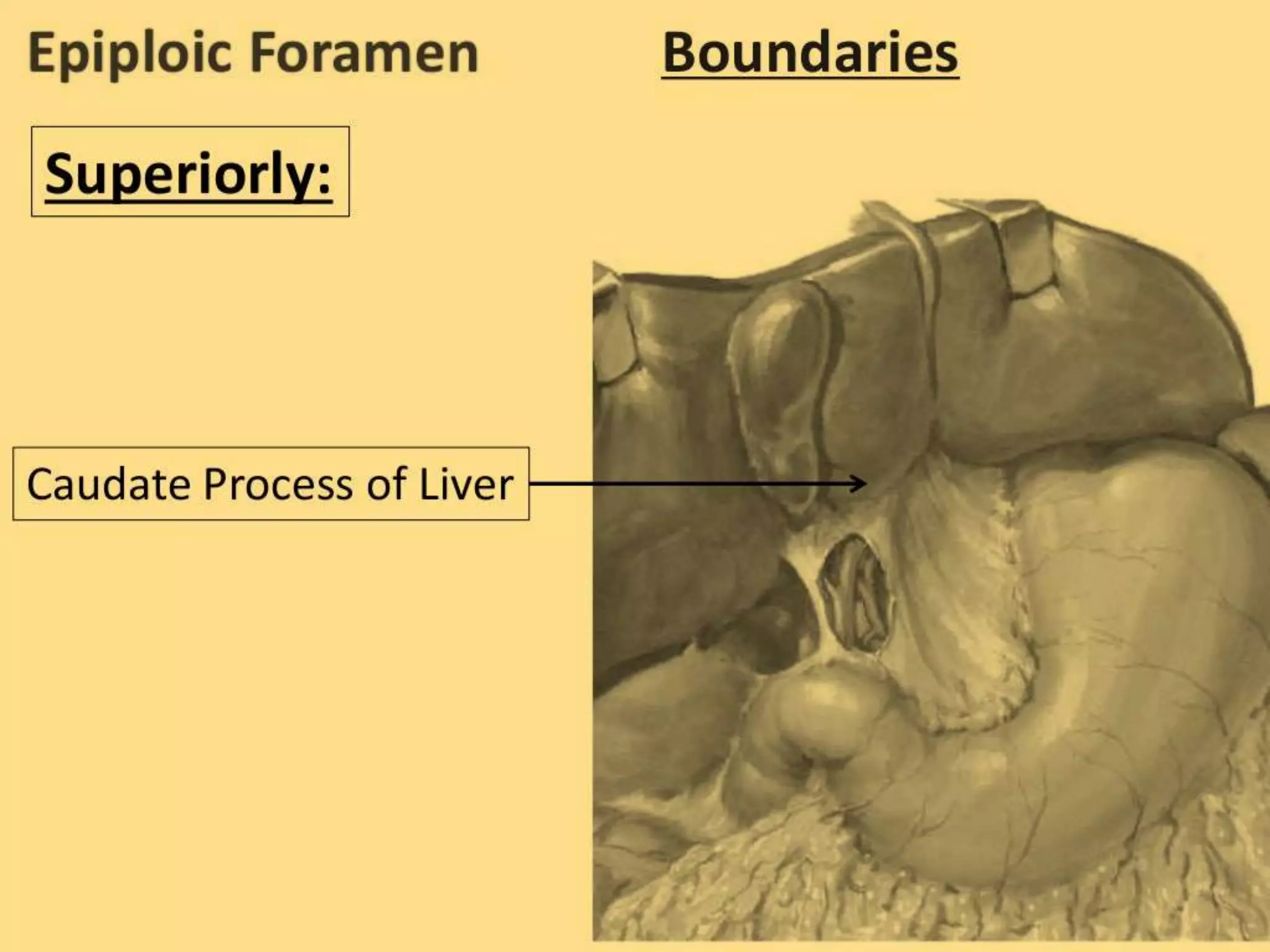

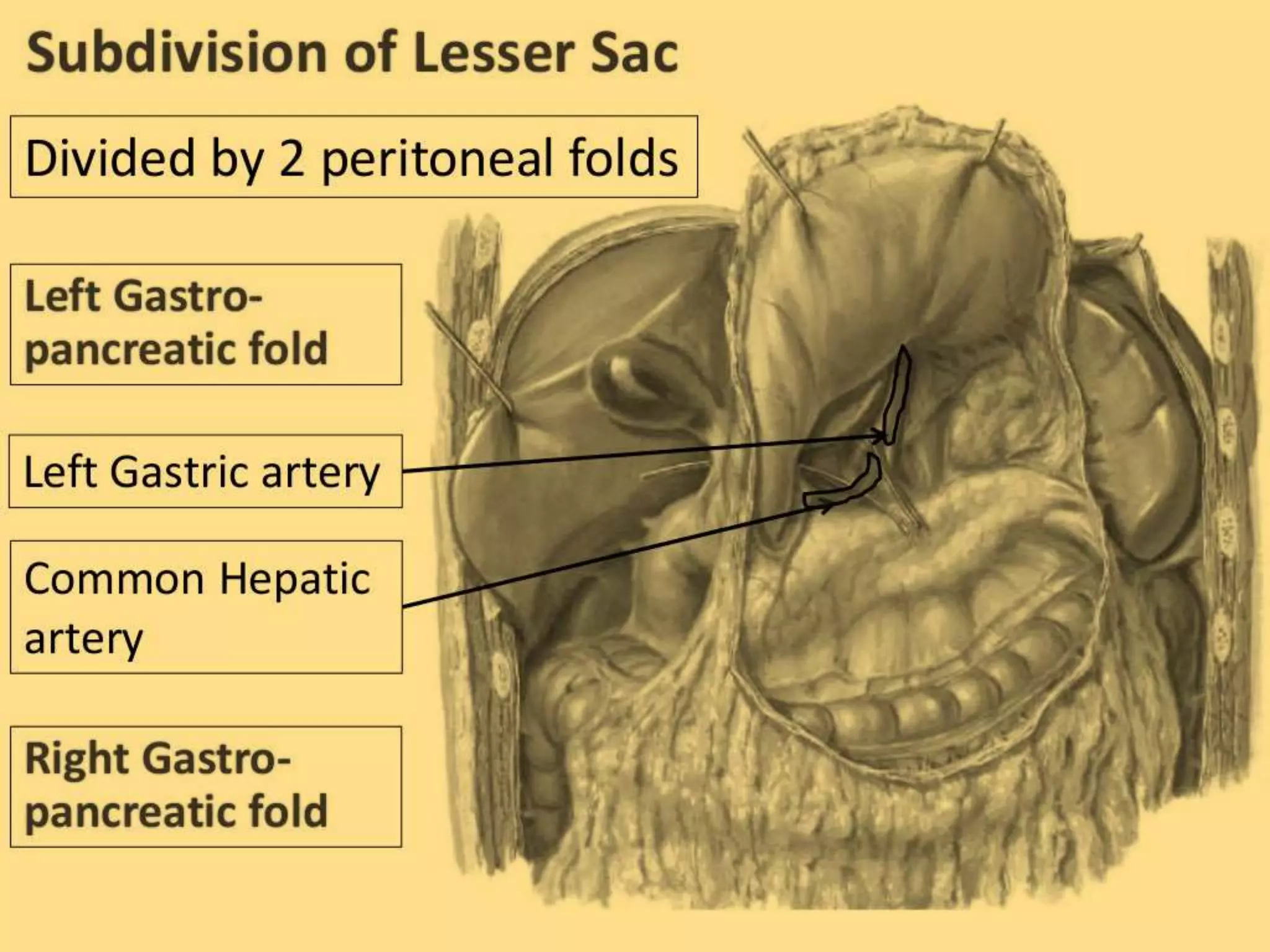





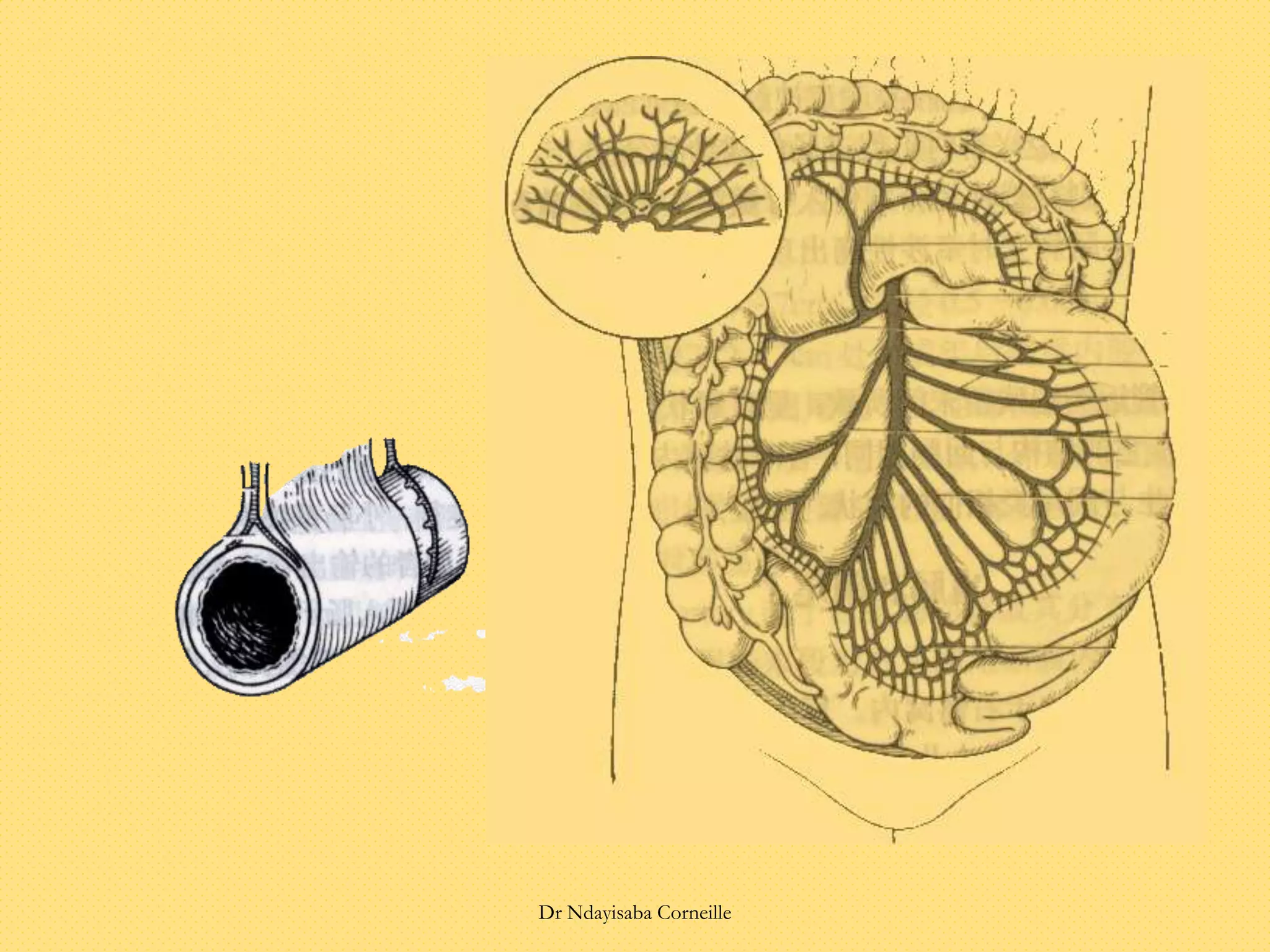











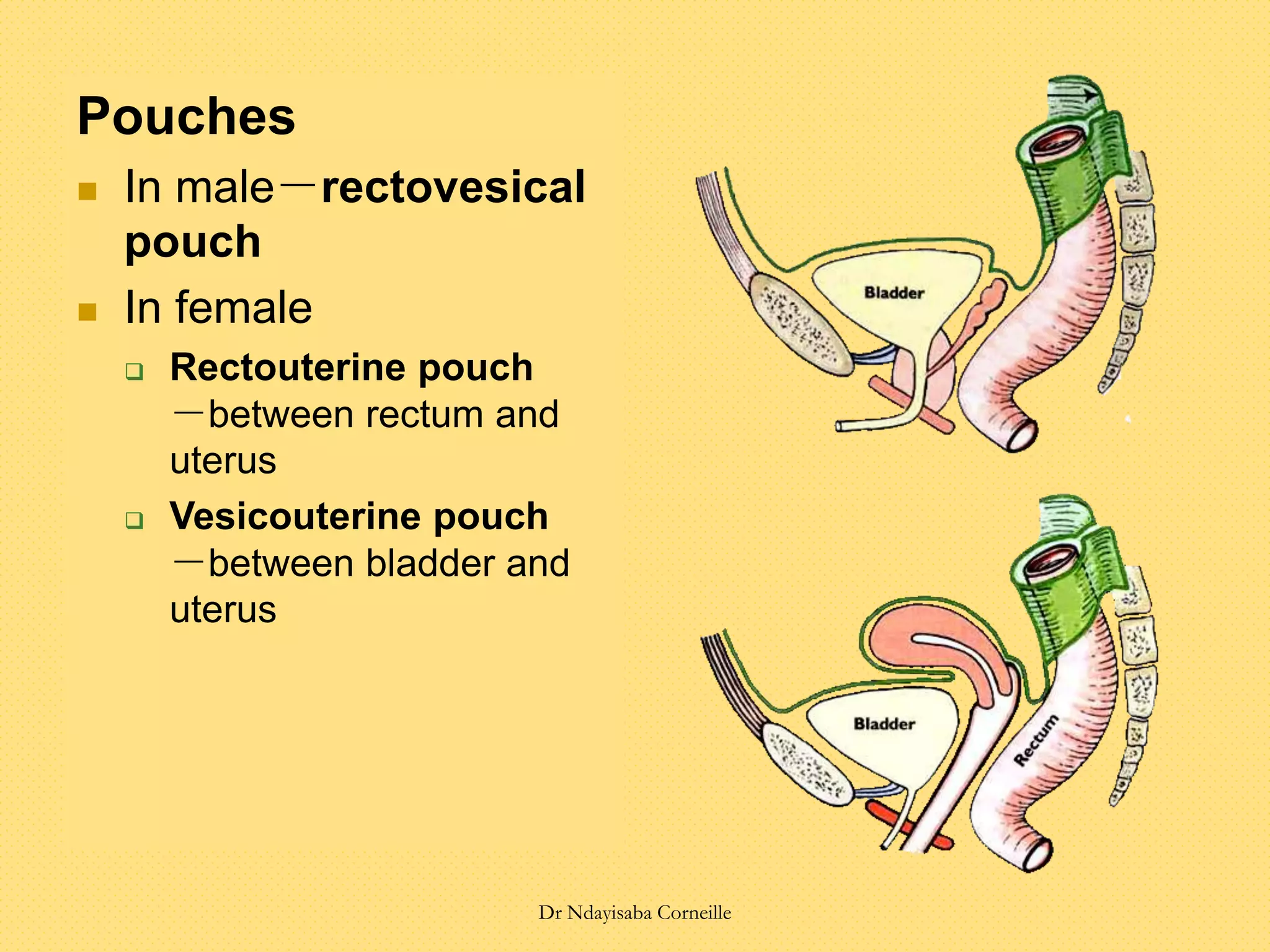
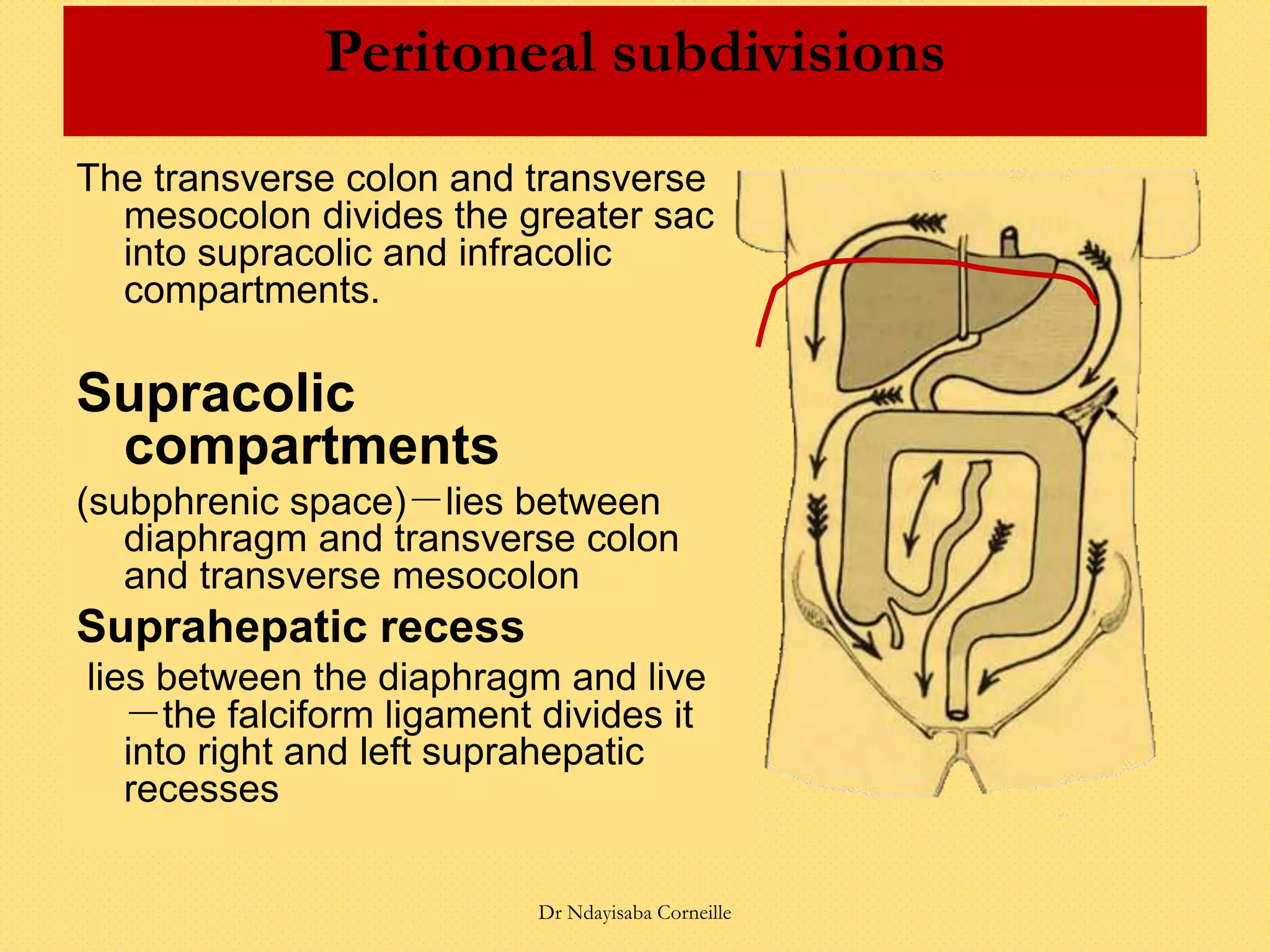

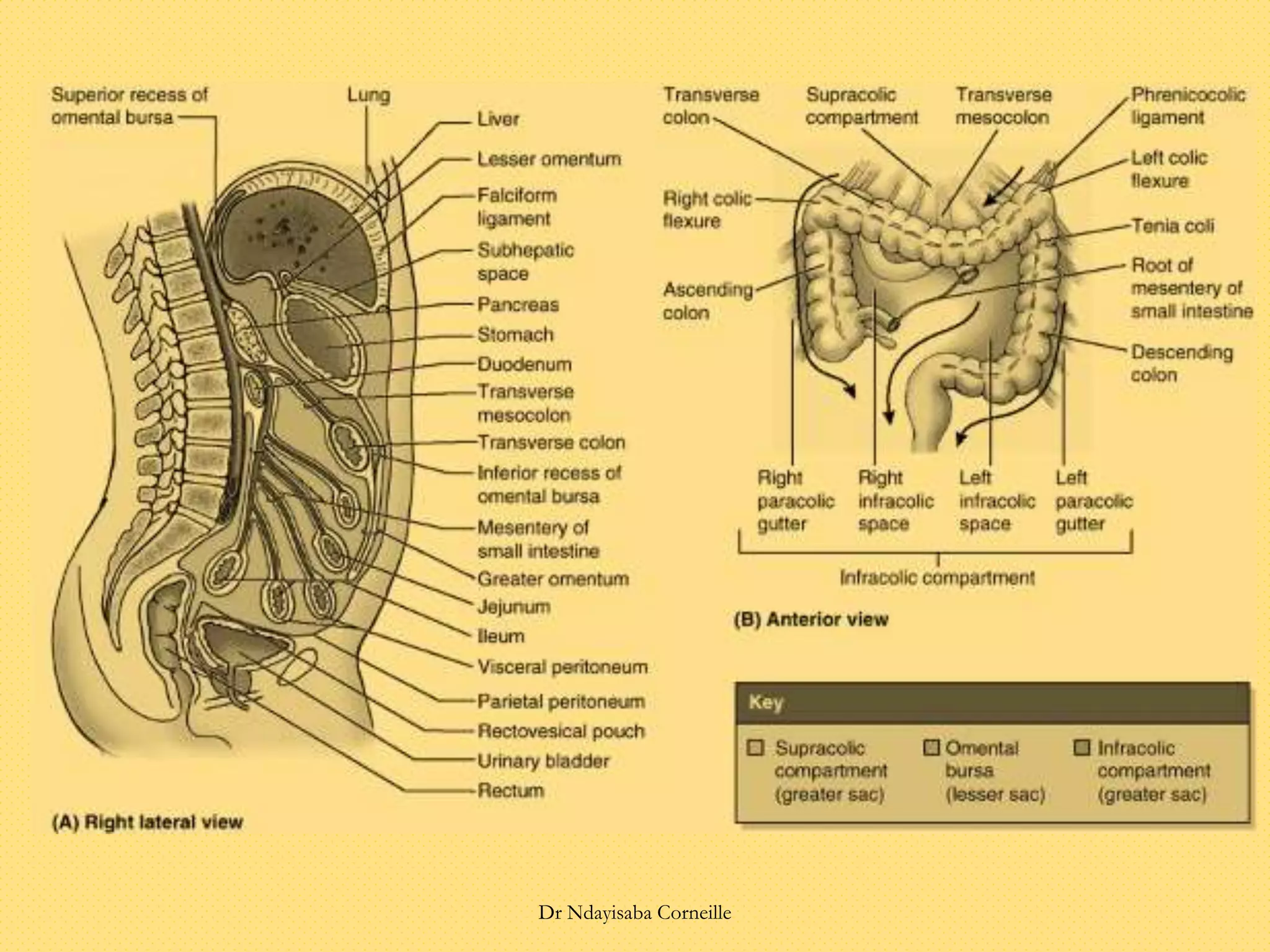
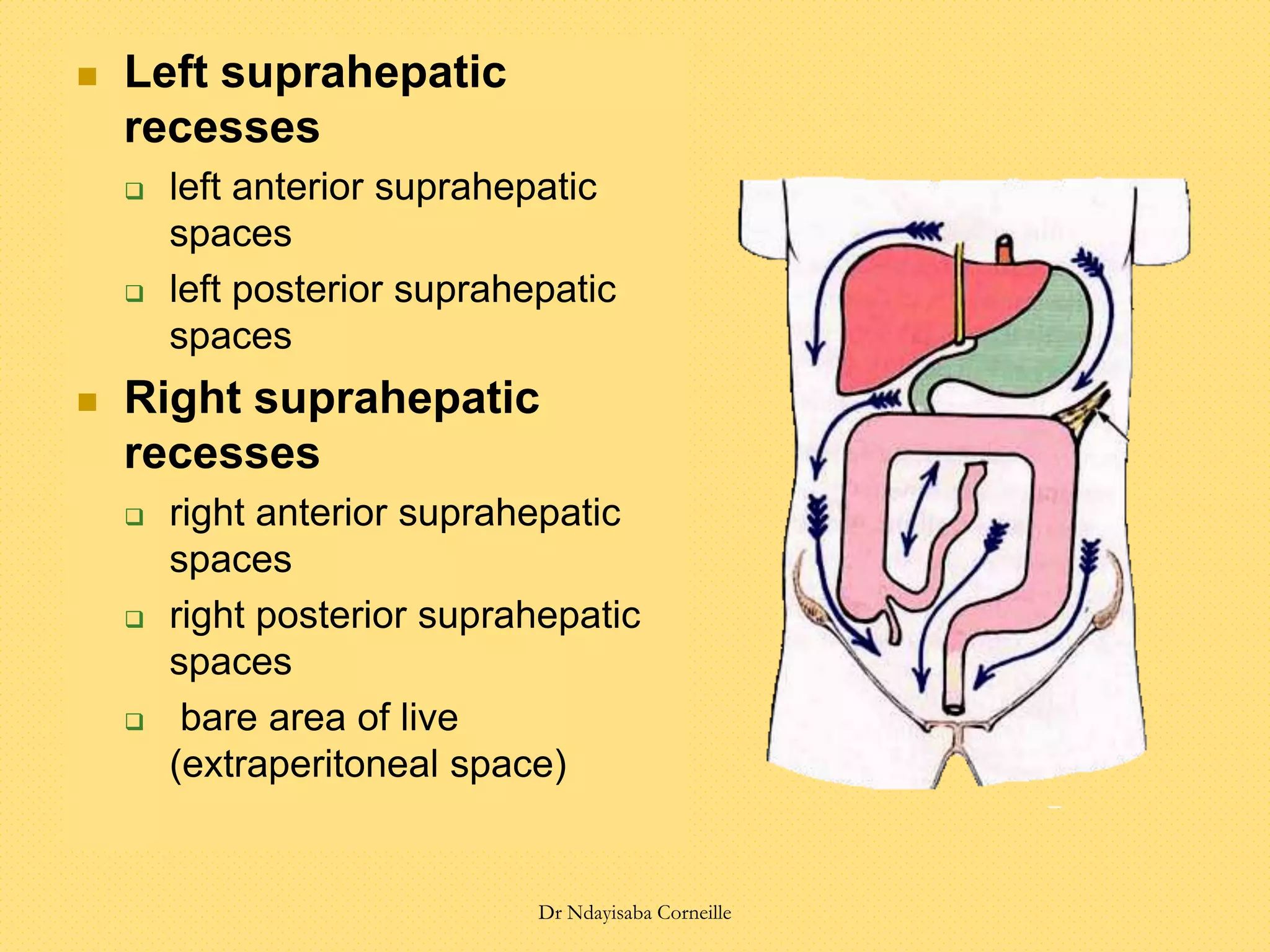

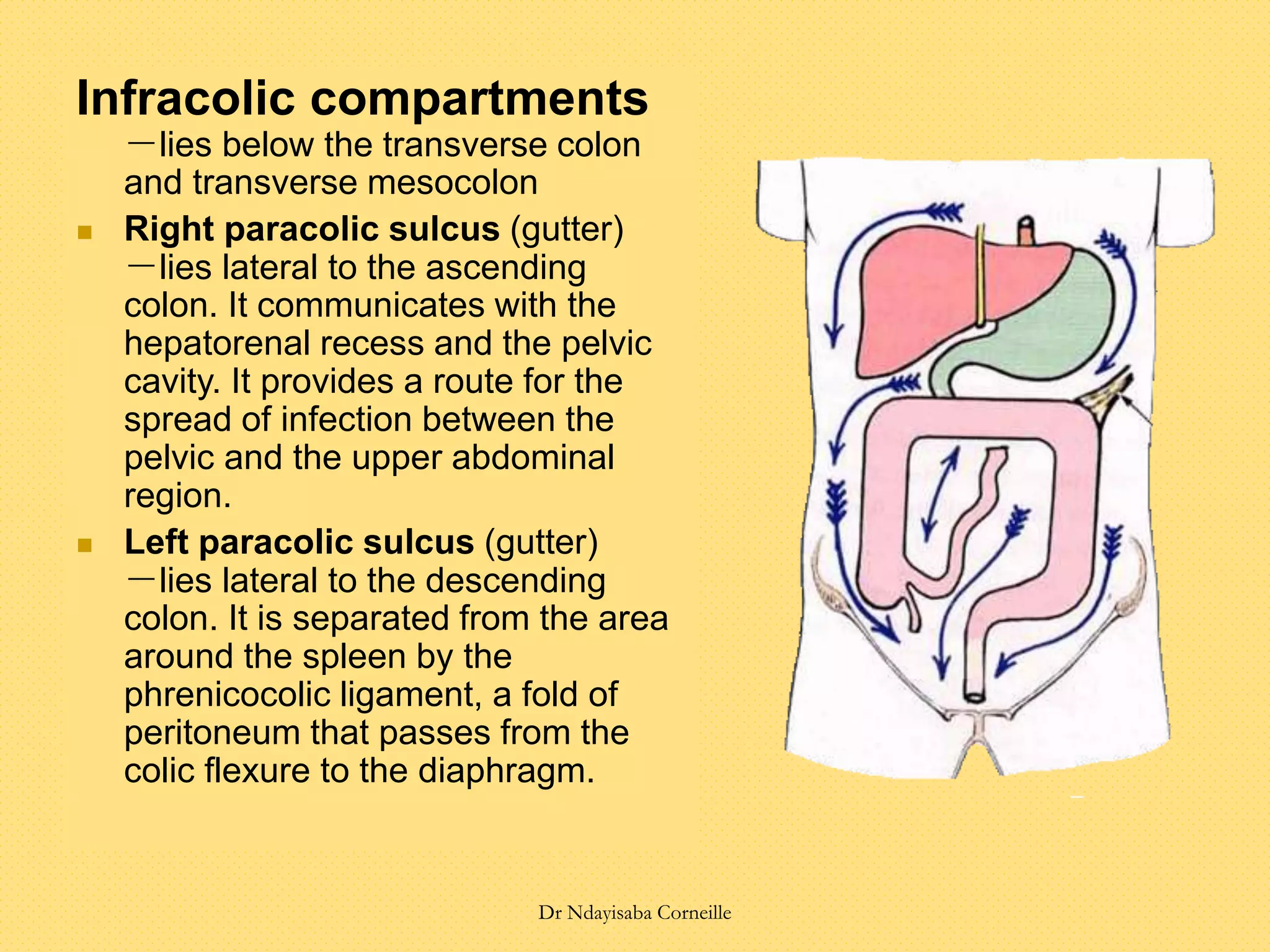


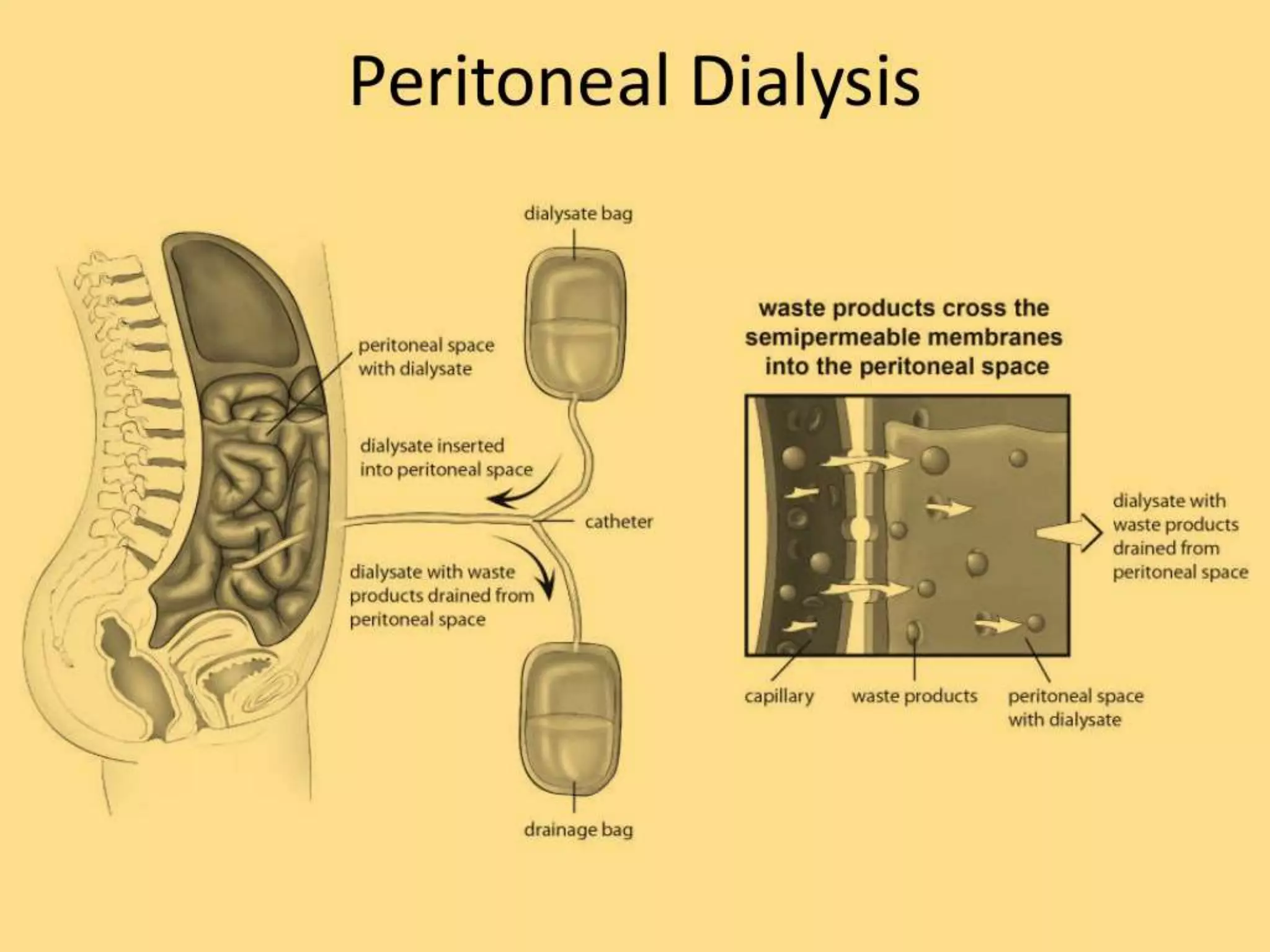
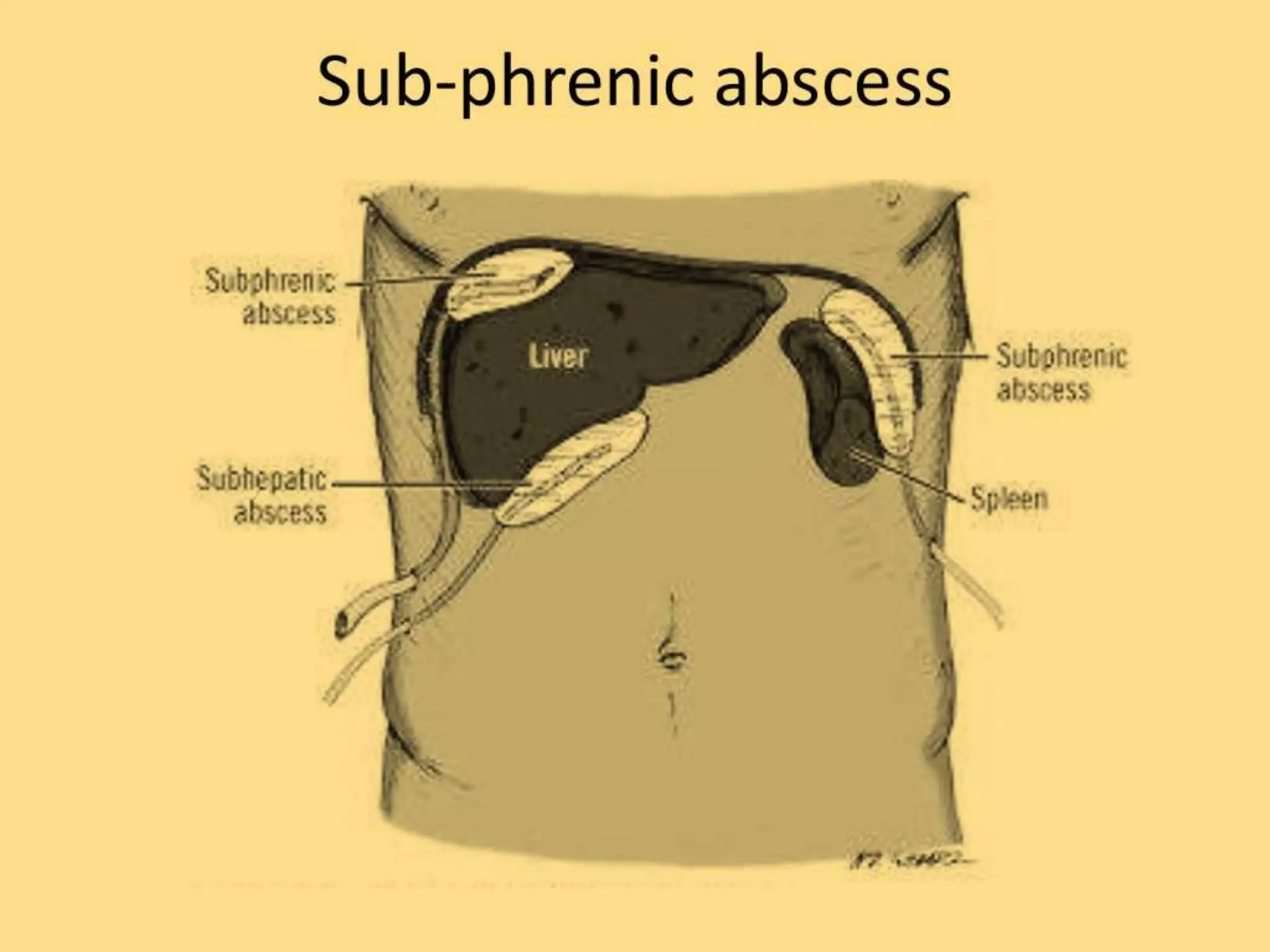


The document discusses the anatomy and relationships of the organs with the peritoneum, categorizing organs into intraperitoneal, interperitoneal, and retroperitoneal based on their coverage by peritoneum. It explains various peritoneal structures such as ligaments, omenta, mesenteries, and pouches, outlining their functions and anatomical significance. Additionally, the document addresses clinical aspects like peritoneal dialysis, internal abdominal hernias, and abdominal pain related to the peritoneum.























































































