Downloaded 311 times

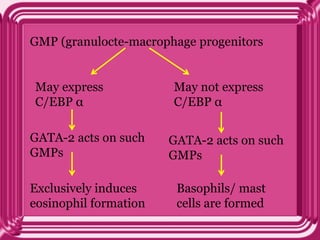






This document provides information on eosinophils: - Eosinophils are white blood cells that are characterized by distinctive granules and a bilobed nucleus. They play a role in fighting parasites and allergic responses. - Eosinophils develop from bone marrow stem cells and are regulated by cytokines like IL-5, IL-3 and GM-CSF. Transcription factors like C/EBP, GATA-1 and PU.1 are required for eosinophil development. - Eosinophils traffic to tissues where they can persist for over a week. Their granules contain toxic proteins that are released during degranulation which is regulated by cytokines and chemokines. - Eosin



































































































