Downloaded 230 times


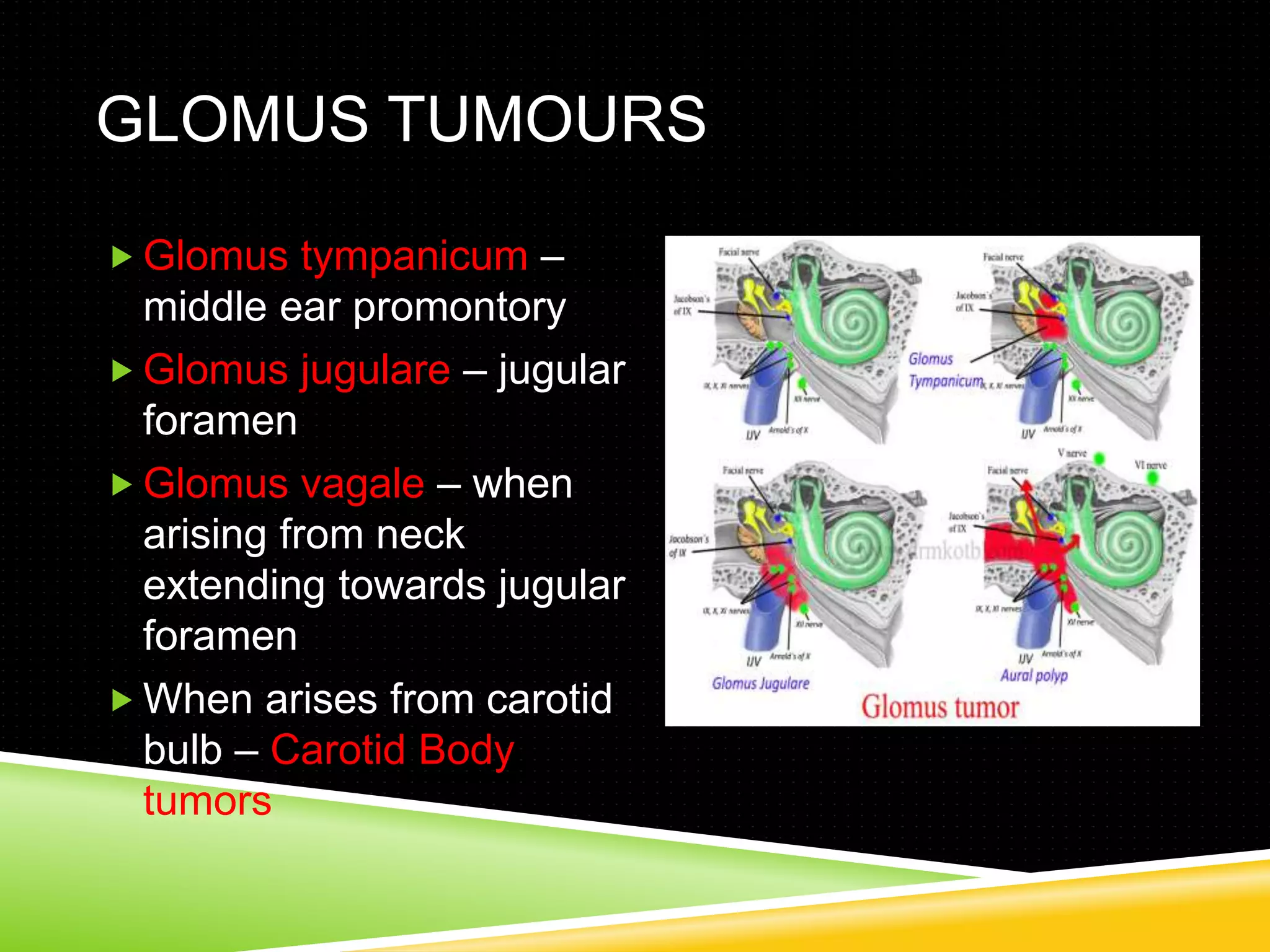


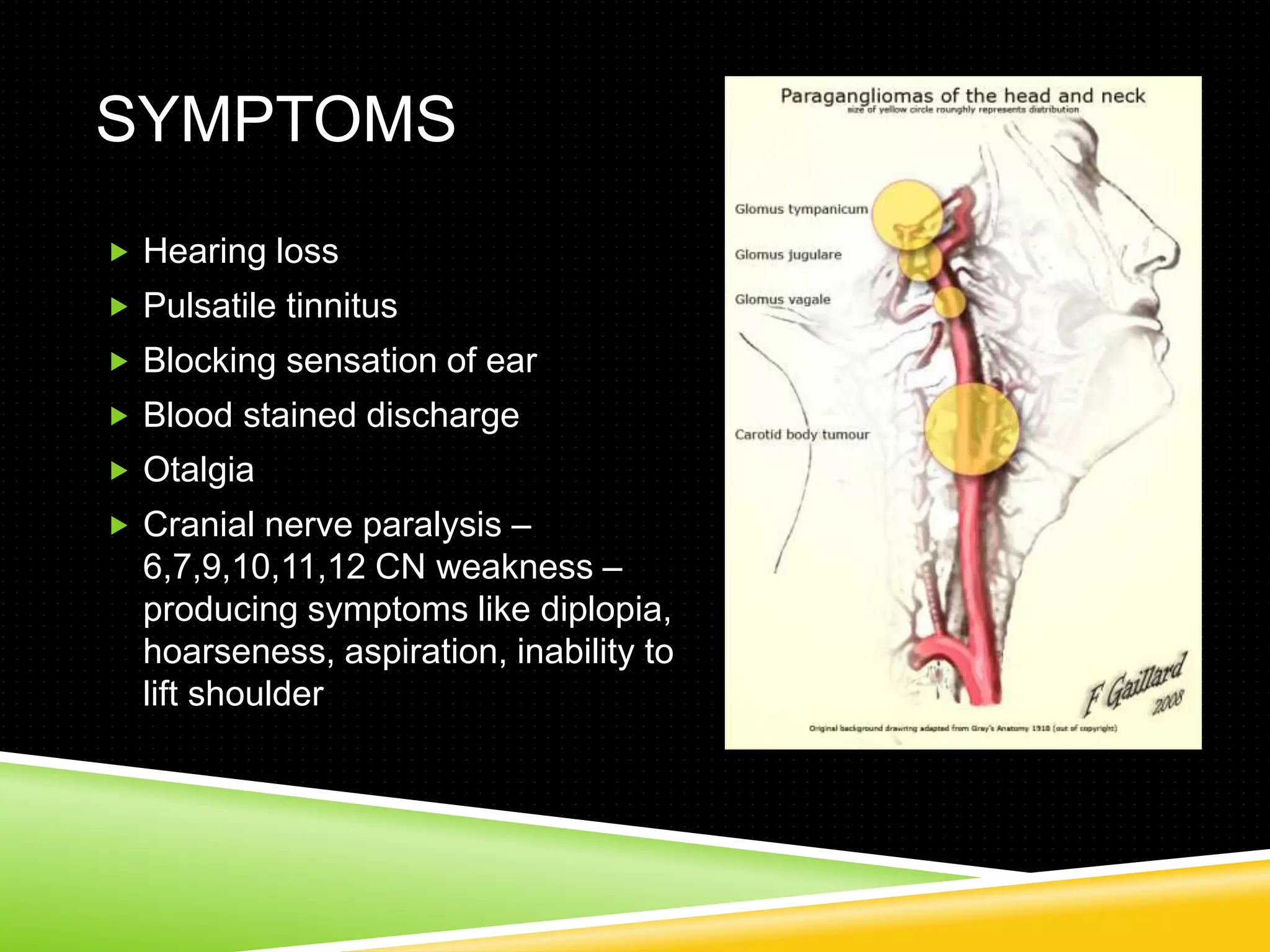

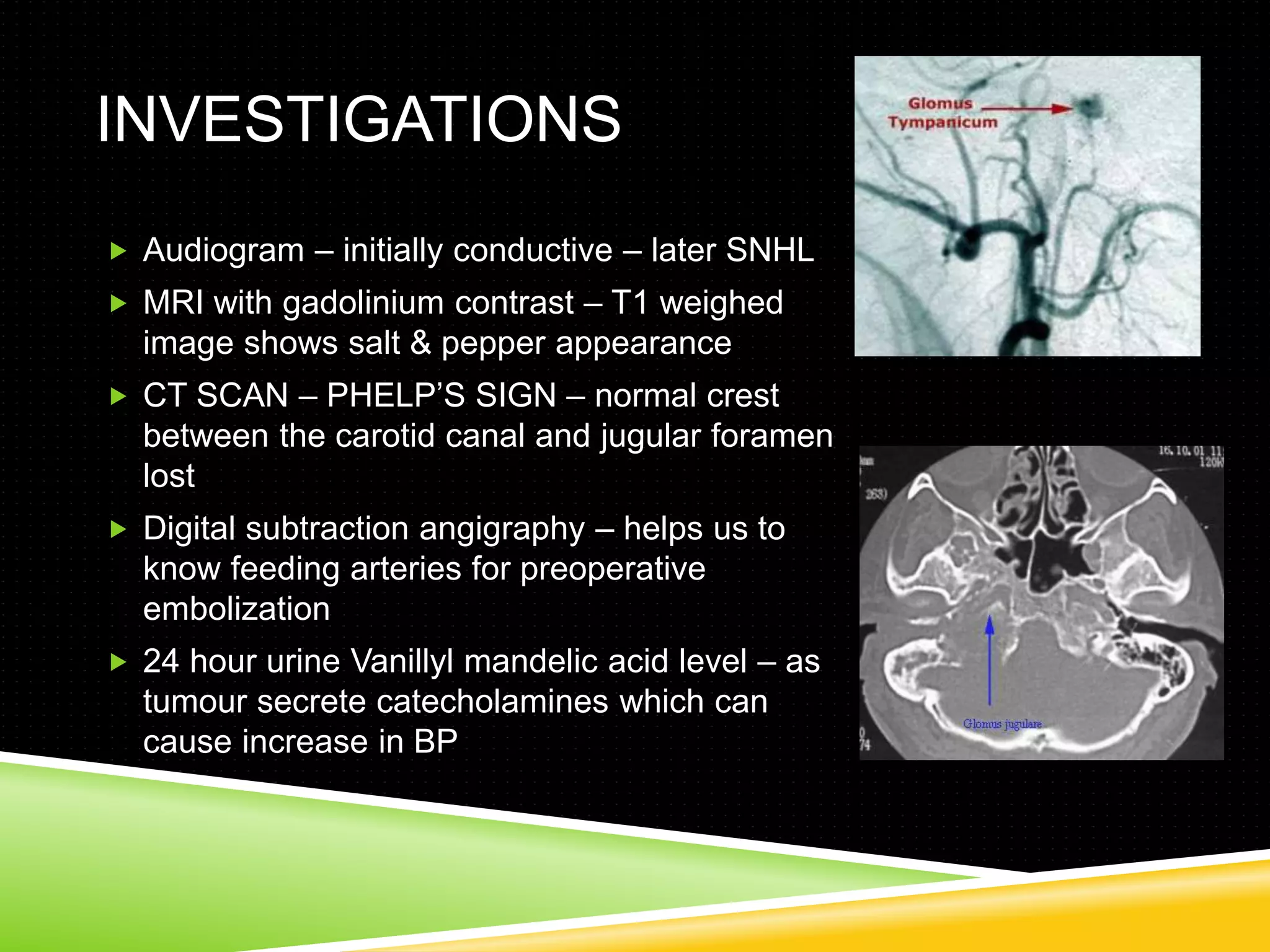


This document discusses glomus tumors, which are rare, hypervascular tumors that arise from glomus bodies. They most commonly occur in the middle ear, jugular foramen, or neck regions. Symptoms depend on location but may include hearing loss, tinnitus, and cranial nerve deficits. Diagnosis involves imaging like MRI and CT. Surgery is the primary treatment and approach depends on tumor size and involvement. Preoperative embolization can help reduce bleeding risk during removal of these vascular tumors.











































































































