Downloaded 21 times
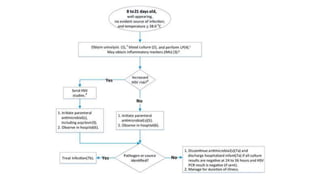
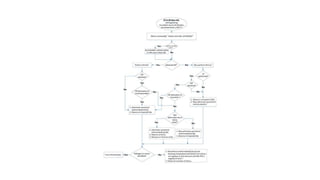


This document discusses the evaluation and management of fever in children. It outlines common causes of fever like viral upper respiratory infections, acute otitis media, pneumonia, urinary tract infections, and meningococcal disease. It emphasizes the importance of distinguishing between well children with common viral illnesses versus those at high risk of serious bacterial infection who require prompt treatment or hospitalization. A thorough history, physical exam assessing for signs of toxicity, and initial lab tests are recommended to diagnose the cause of fever and guide appropriate management.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







