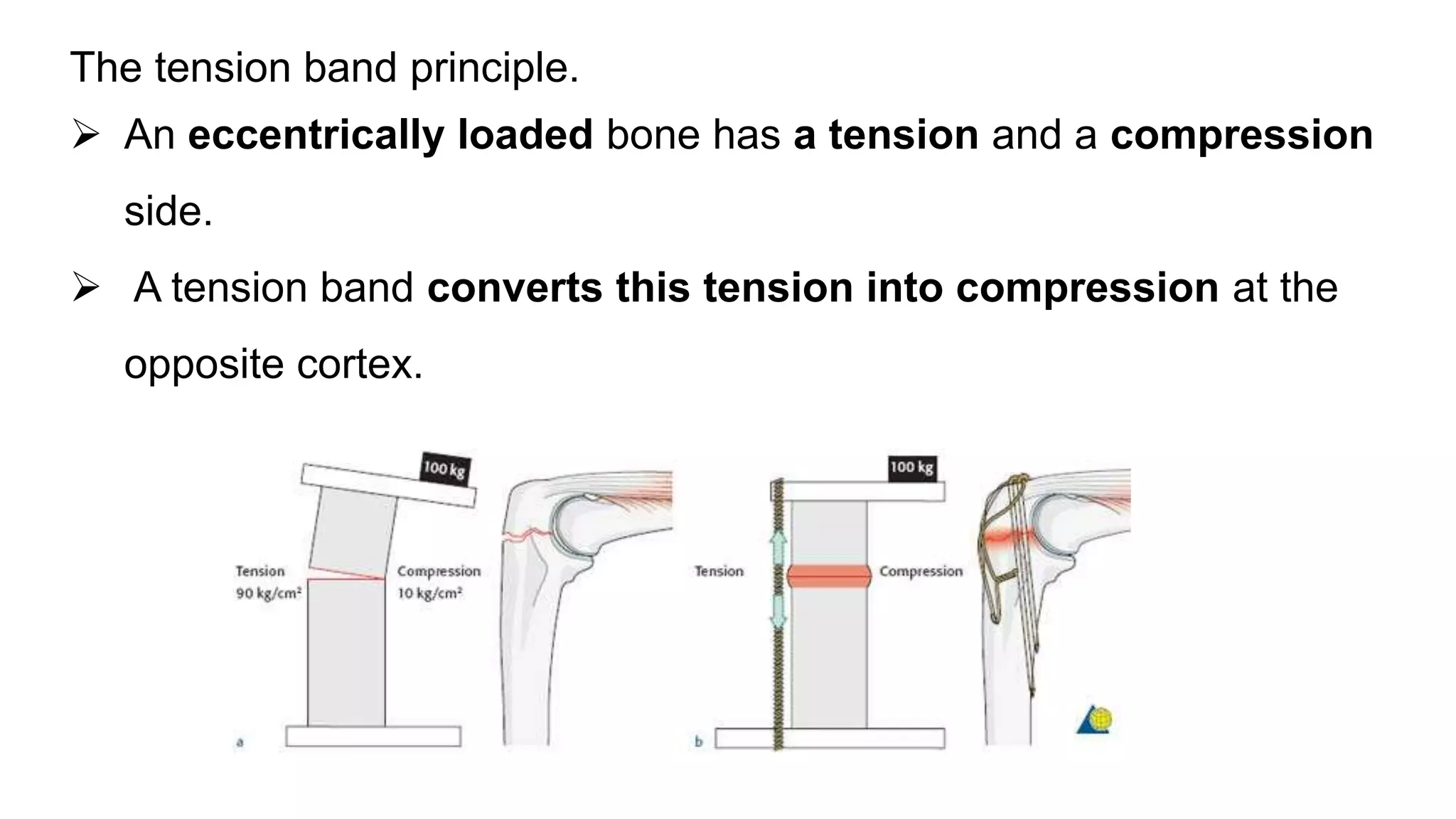
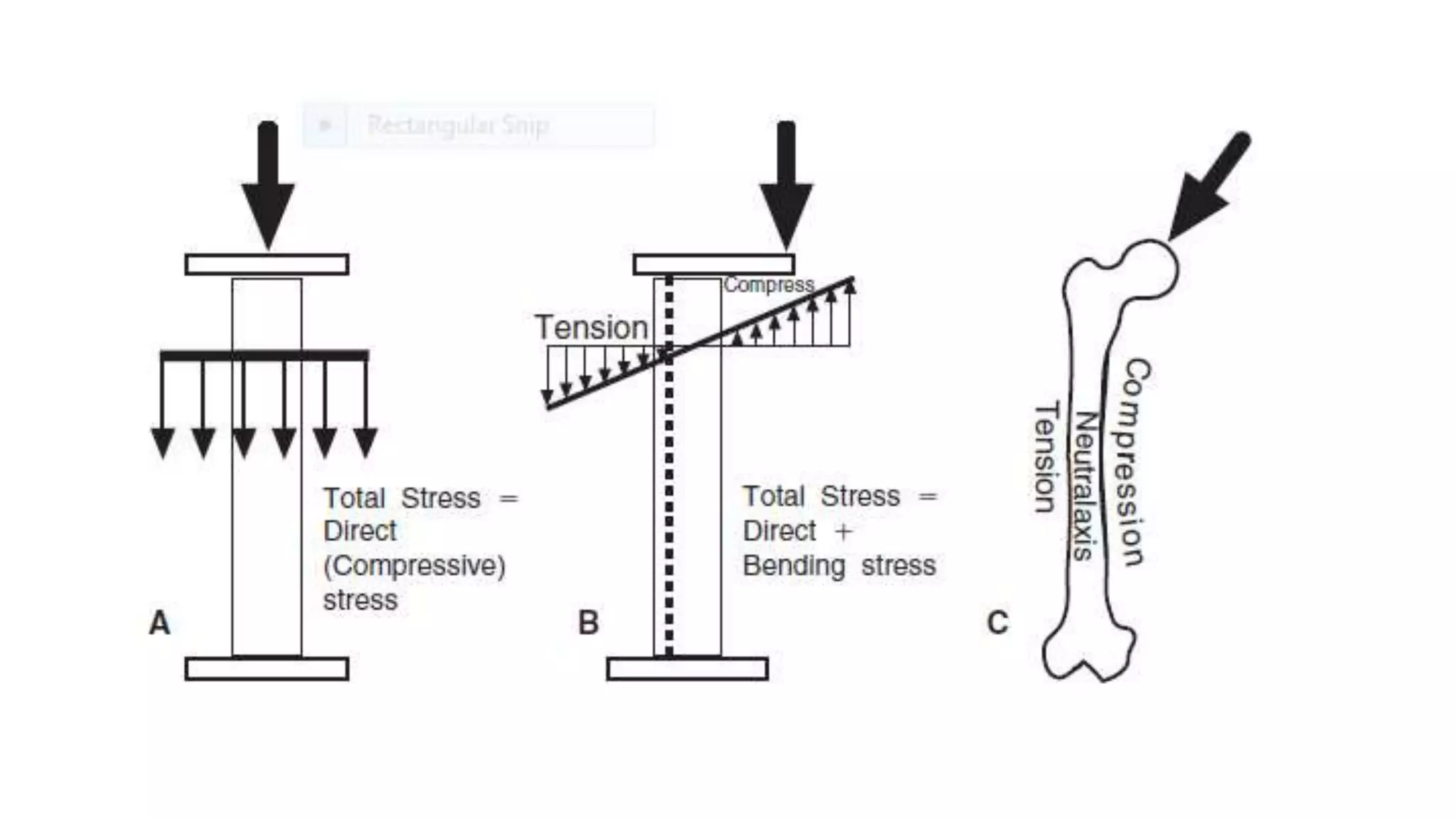
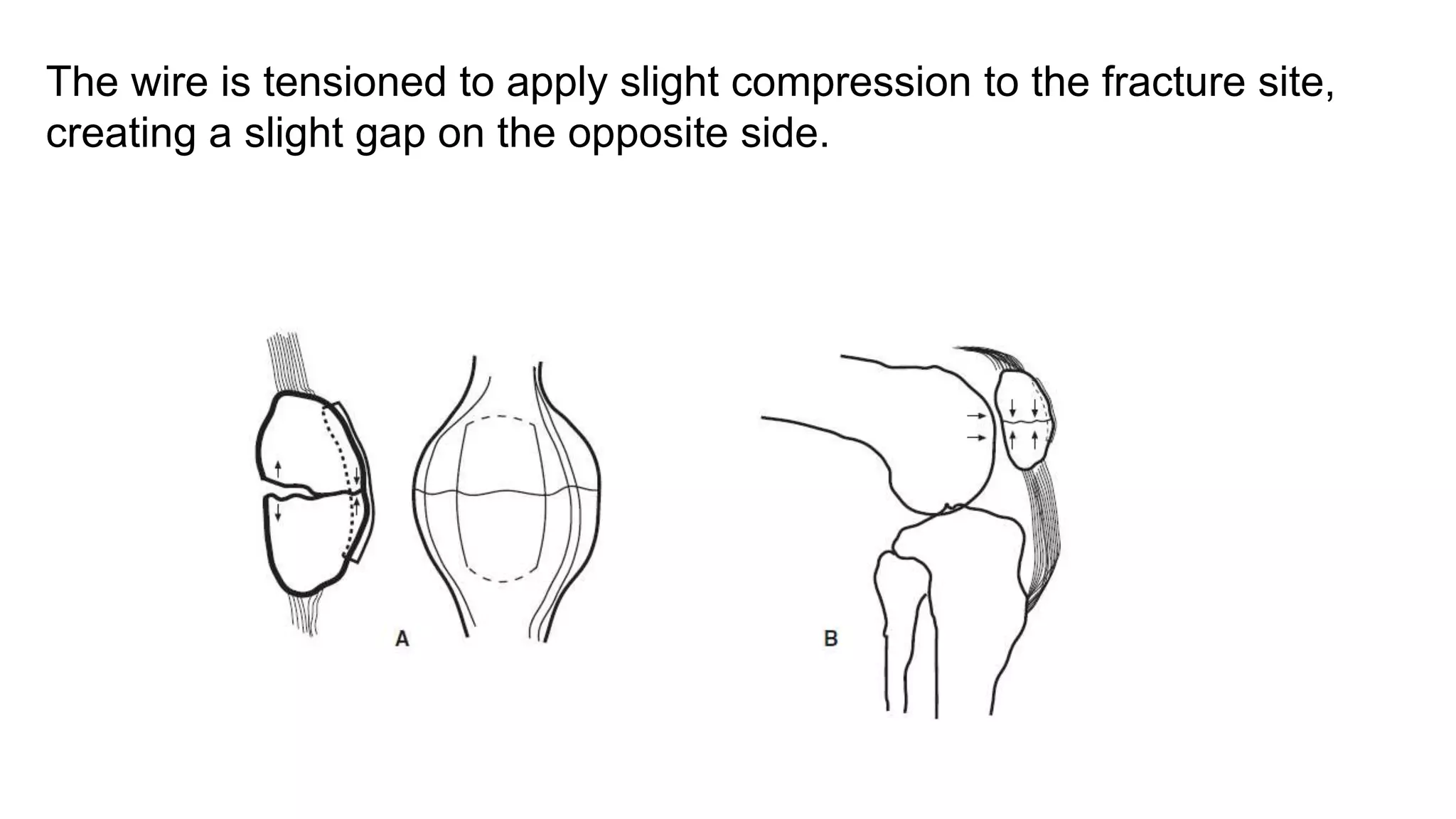
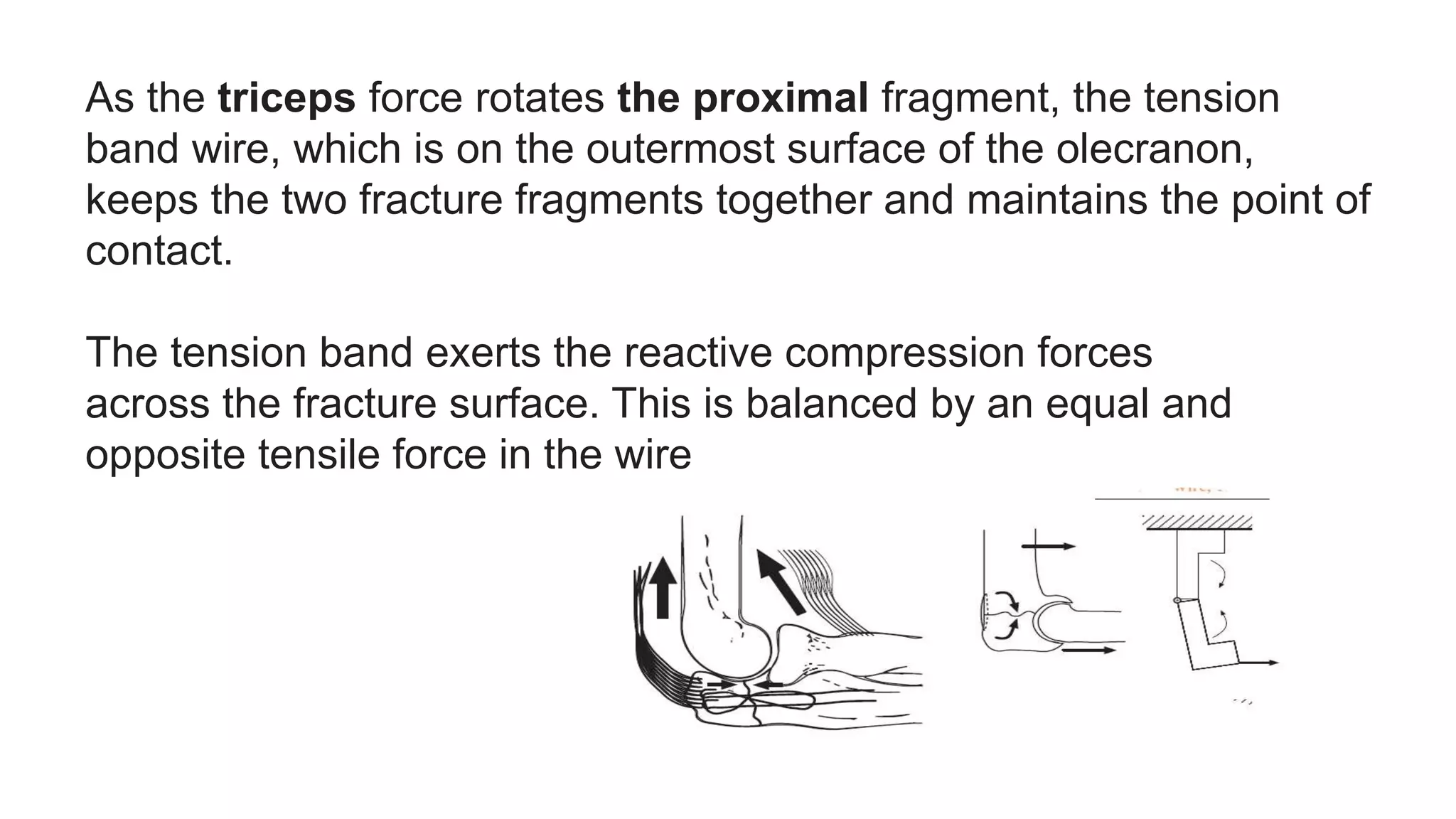
The document discusses the principles and applications of tension band wiring in orthopedic surgery, detailing how it converts tensile forces into compressive forces to aid in bone healing. It highlights the importance of proper wire application, material selection, and the specific types of fractures suitable for this technique. Additionally, the document outlines potential complications, including implant failure and wire prominence issues.










































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











