Download as PDF, PPTX



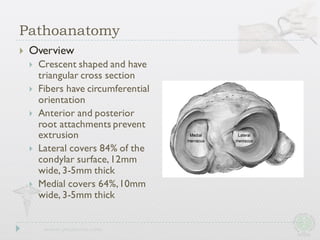
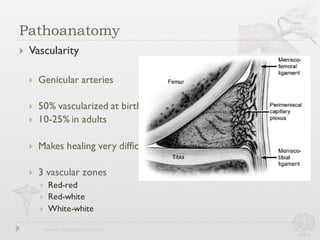
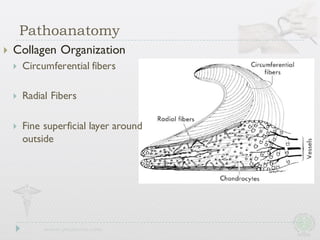


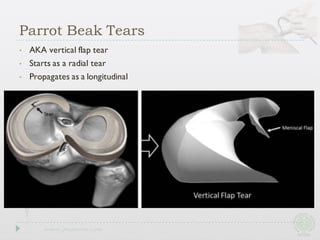














This document discusses meniscal tears, including types of tears, anatomy, function, biomechanics, diagnosis, and treatment options. It provides an overview of the meniscus, noting its crescent shape, fibers, and vascularity. Types of tears include longitudinal, radial, horizontal, complex, and bucket handle tears. Diagnosis involves physical exam maneuvers like McMurray's test and imaging like MRI. Treatment options discussed include arthroscopic partial meniscectomy, open or arthroscopic repair, and all-inside repair techniques. Outcomes and complications of procedures are also summarized.









































![MENISCUS 2745236382575687647634TEAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/meniscustear1-251213165858-d2427fa8-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















