This document provides an overview of the temporomandibular joint (TMJ), including its:
- Types (synovial, bicondylar, ginglymoarthroidal)
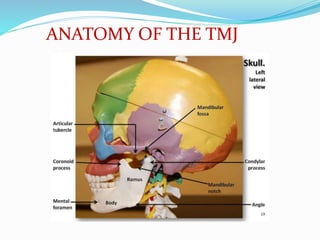
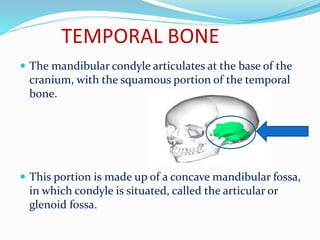
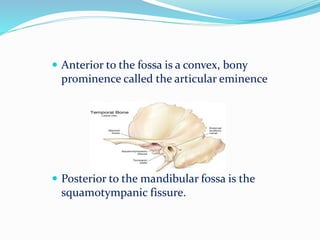
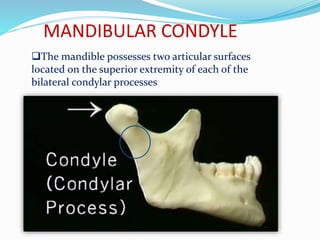
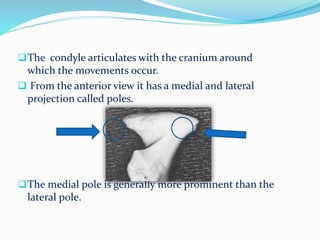
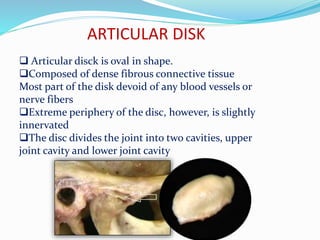
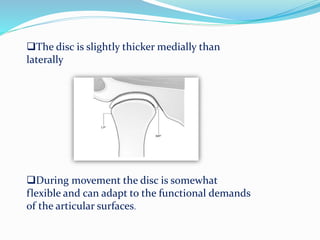
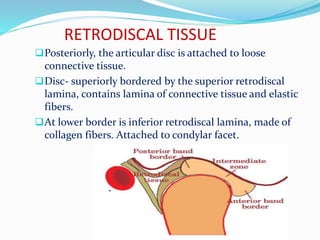
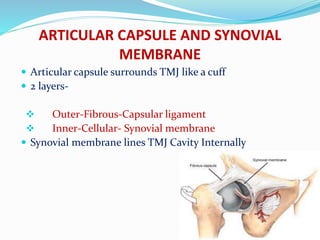
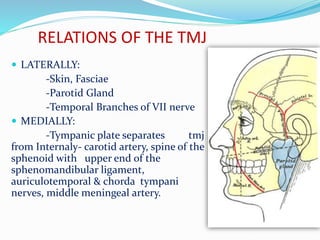
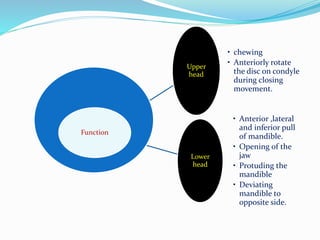
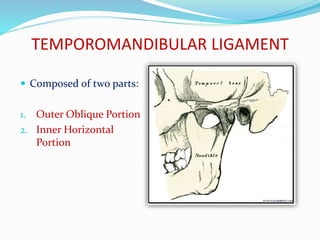
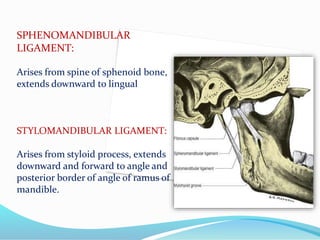
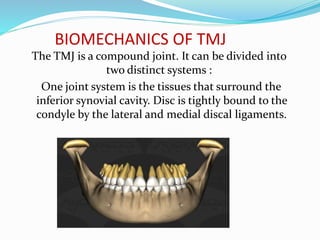
- Anatomy (bones, articular disc, ligaments, muscles)
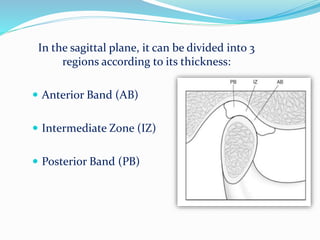
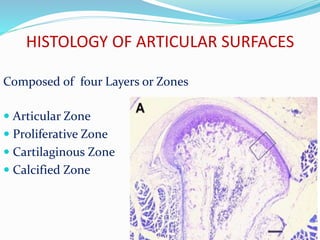
- Histology of the articular surfaces
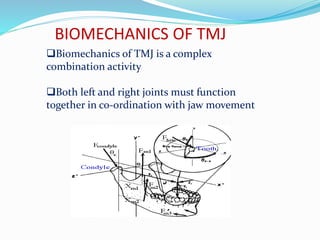
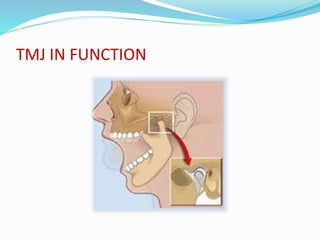
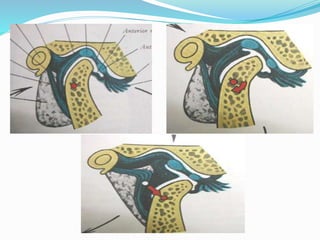
- Biomechanics and functions like opening and closing the mouth
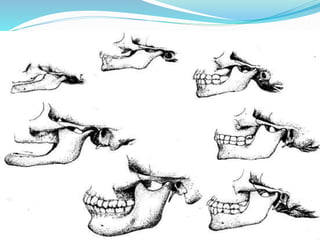
- Age-related changes like flattening of bones and thinning of tissues

















































![Temporomandibular joint [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/temporomandibularjointautosaved-230521065437-1cbd4148-thumbnail.jpg?width=640&height=640&fit=bounds)













































