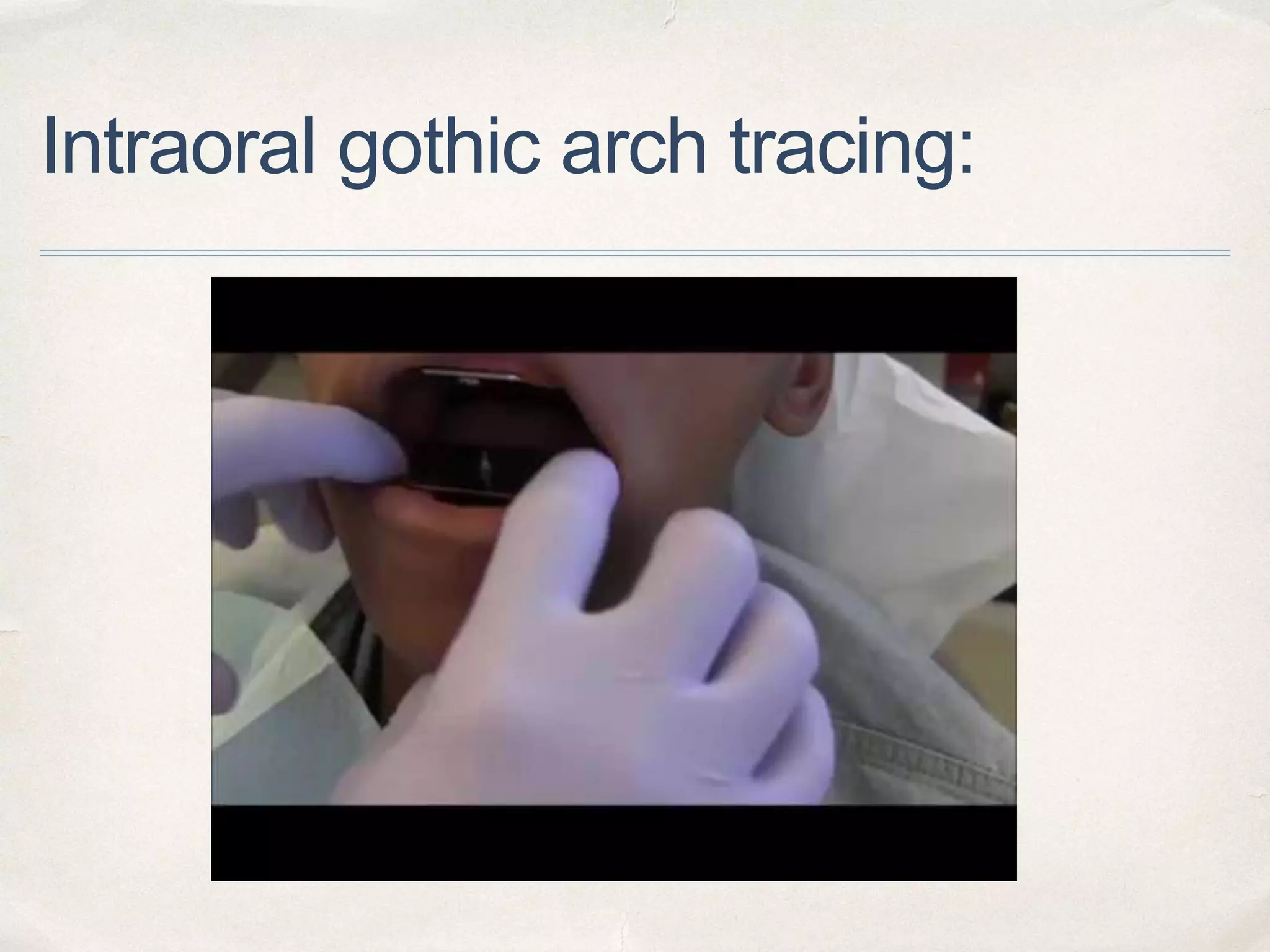
This document provides an overview of Gothic arch tracing techniques used to record centric relation. It defines key terms and discusses the history and evolution of graphic recording methods from early needle point tracings to modern extraoral and intraoral tracers that produce Gothic arch tracings. The conventional extraoral technique is described in 12 steps, from mounting the tracers to making centric and protrusive plaster records. Intraoral tracings are noted to be smaller and harder to observe during tracing compared to extraoral methods.















![References
1. Glossary of prosthodontic terminologies, 9th edition.
2. Keshvad A, Winstanley RB. An appraisal of the literature on centric relation. Part III. J Oral Rehabil 2001;28:55-63
3. Wilson PHR, Banerjee A. Recording the re- truded contact position: a review of clinical techniques. Br Dent J 2004;196:395-
402.
4. Bansal S, Palaskar J,The Journal of Indian Prosthodontic Society | December 2008 | Vol 8 | Issue 4, 10.4103/0972-
4052.49180
5. Babita Y et al / Int. J. of Allied Med. Sci. and Clin. Research Vol-3(3) 2015 [308-312].
6. Myers M, Dziejma R, Goldberg J, Ross R, Sharry J. Relation of Gothic arch apex to dentist-assisted centric relation. J Prosthet
Dent 1980;44:78-81.
7. Campos AA, Nathanson D, Rose L. Reproducibility and condylar position of a physiologic maxillomandibular centric relation in
upright and supine body position. J Prosthet Dent 1996;76:282-7.
8. Lundeen HC. Centric relation records: the effect of muscle action. J Prosthet Dent 1974;31-3:244-53.
9. Dawson PK. Evaluation, diagnosis, and treatment of occlusal problems.2nd ed. St Louis: CV Mosby; 1989. p. 41-169.
10.Langer A, Michman J. Intraoral technique for recording vertical and horizontal maxillomandibular relations in complete
dentures. J Prosthet Dent. 1969;21:599-606.](https://image.slidesharecdn.com/11-201020113830/75/Gothic-arch-tracing-38-2048.jpg)










































































