Downloaded 58 times
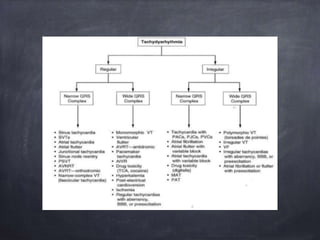
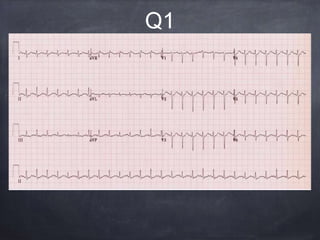
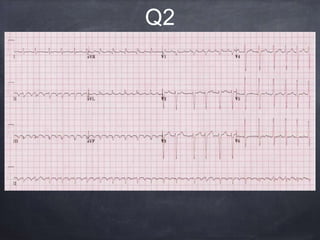
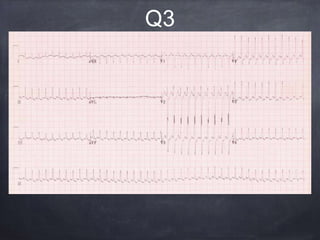
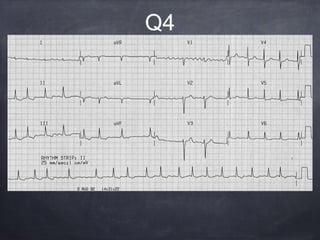
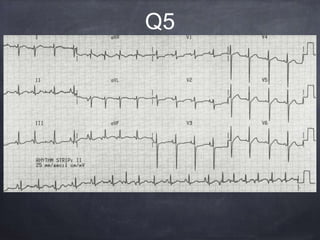
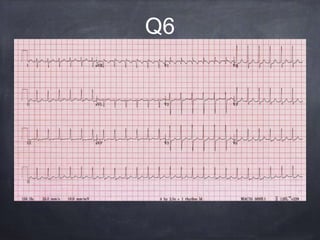
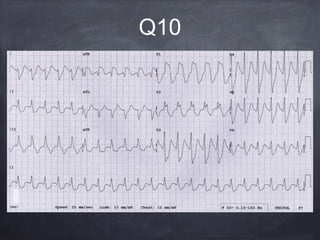
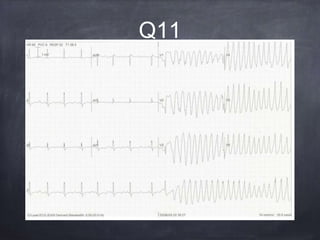
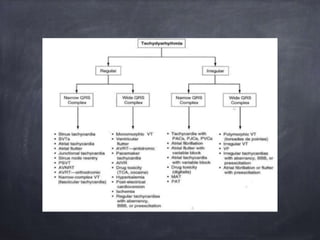
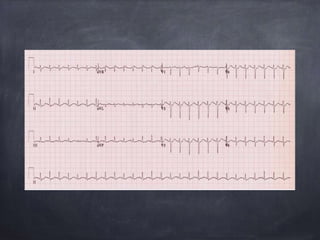
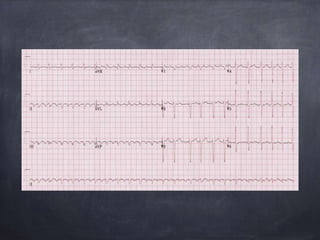
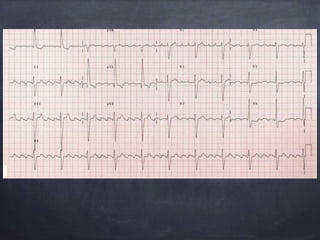
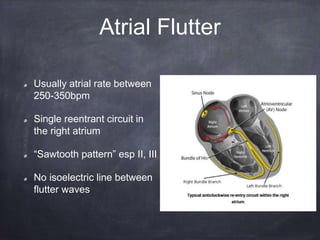
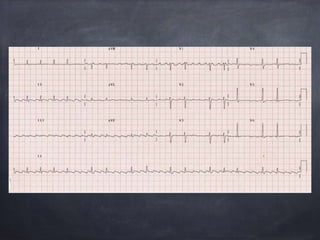
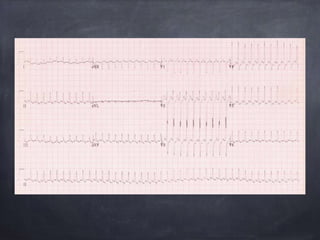
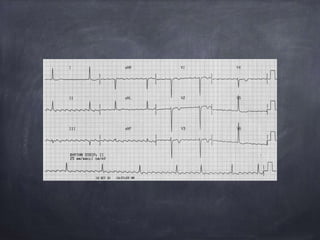
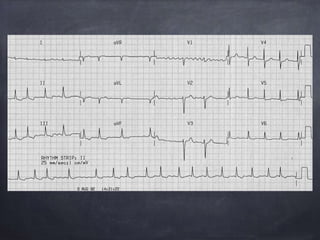
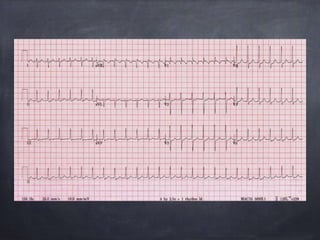
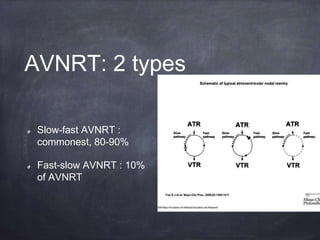
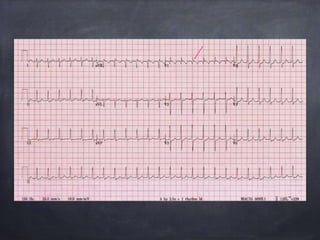
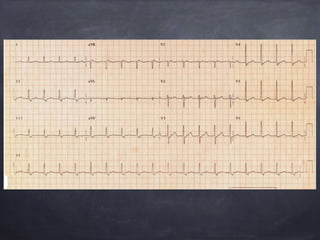
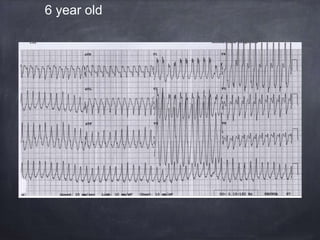
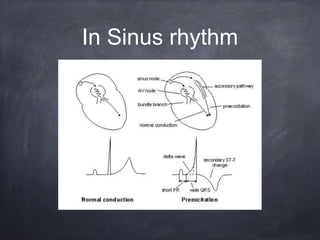
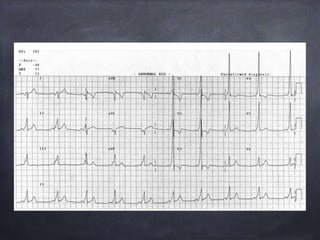
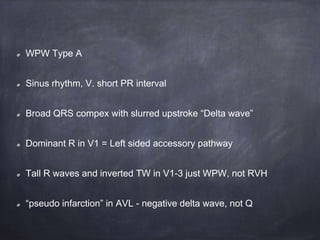
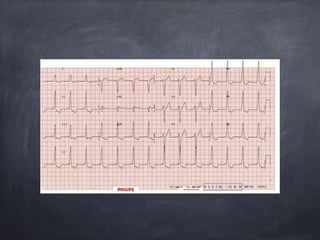
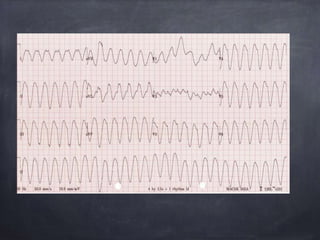
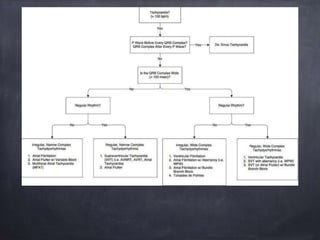

This document discusses various tachyarrhythmias including: - Sinus tachycardia with a rate usually between 100-160 bpm. - Atrial flutter with a typical sawtooth pattern and ventricle rate between 65-150 bpm depending on block. - Atrial fibrillation seen as irregularly irregular rhythm with fibrillatory waves in leads. - AV nodal reentrant tachycardia (AVNRT) being the most common form of supraventricular tachycardia, with retrograde P waves sometimes hidden in QRS. - Wolff-Parkinson-White syndrome seen as a short PR interval with slurred QRS upstroke in sinus rhythm























































































