Downloaded 64 times
















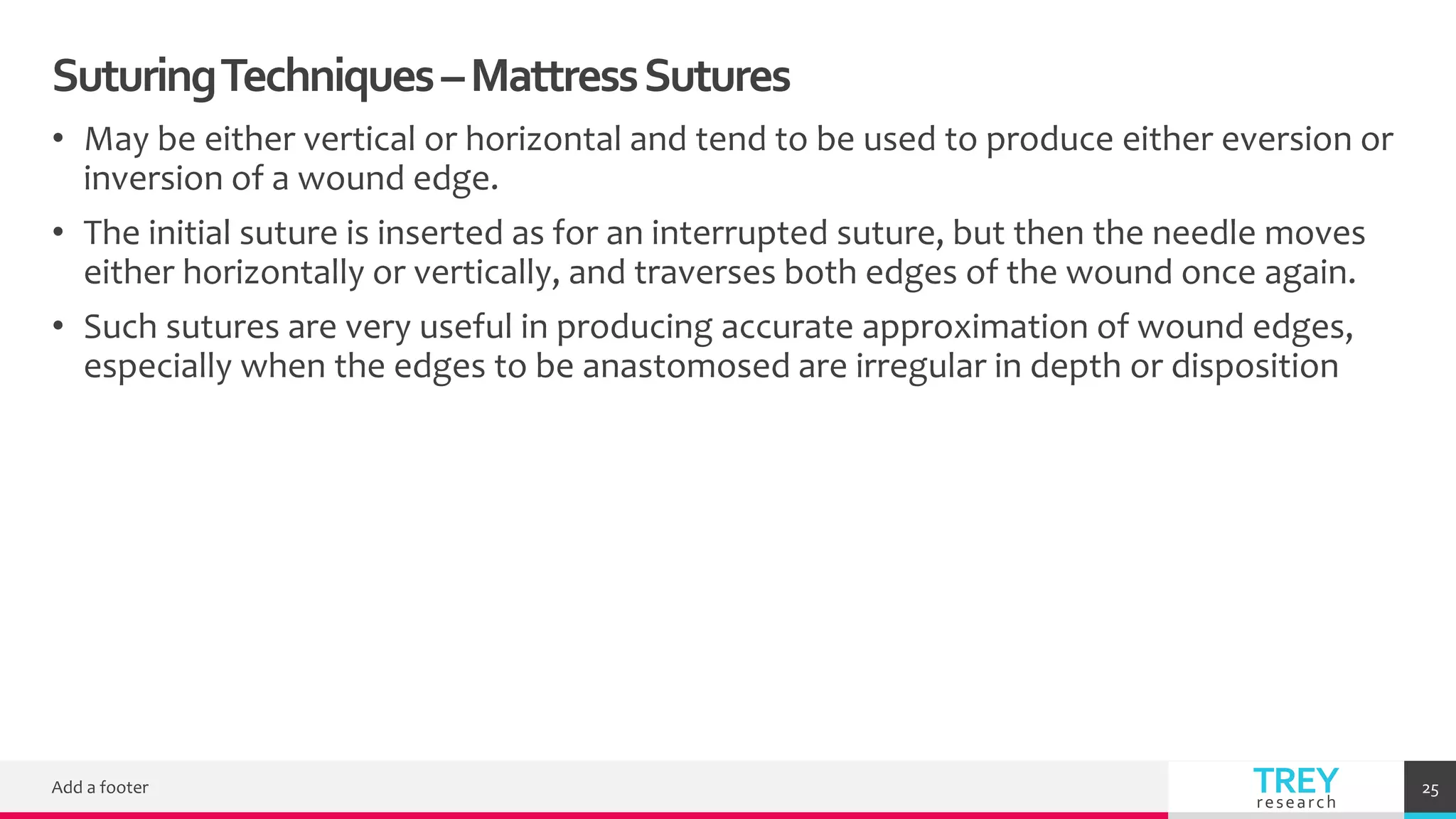











This document discusses wound closure, suturing techniques, and suture materials. It provides details on ideal characteristics of suture materials, different suture characteristics like strength and absorbability. It also describes various suturing techniques like simple interrupted, continuous, and mattress sutures. Finally, it discusses alternatives to sutures like skin adhesives, tissue glue, and techniques for laparoscopic wound closure.






















































































