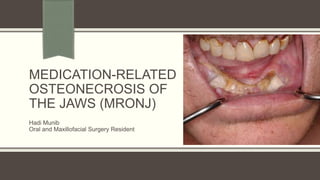
The document provides information on Medication-Related Osteonecrosis of the Jaws (MRONJ). It discusses the AAOMFS definition, predisposing factors like dentoalveolar surgery, staging of MRONJ from 0-3, bisphosphonate medications and recommendations for patients receiving or about to start these medications. It also covers osteomyelitis including classification, pathogenesis, clinical presentation, investigations and surgical management. Overall, the document is an overview of MRONJ and osteomyelitis of the jaws for oral and maxillofacial surgery residents.
A brief description of all topics to recent advances,SDD, host modulation and diabetes, host modulation in smokers, chemically modified tetracyclines, bisphosphonates
A brief description of all topics to recent advances,SDD, host modulation and diabetes, host modulation in smokers, chemically modified tetracyclines, bisphosphonates
Certains medications have been associated with gingival enlargement.
the seminar gives a complete analysis of etilogy and pathogenesis involved in digo as well as sequlae of it
Periodontal risk & making risk assessmentibrahimaziz15
Periodontal risk and risk assessment is very importnant in monitoring periodontally affected patients, this seminar will give you an idea about periodontal risk factors and how to make a periodontal risk assessment for patients.
Systemic Peridoontology, link between systemic health and periodontology, diabetes and periodontology, Pregnancy and Peridotology,Nutrition and periodontology
AGGRESSIVE PERIODONTITIS
PRESENTER
DR. REBICCA RANJIT
DEPT. OF PERIODONTOLOGY & ORAL IMPLANTOLOGY
Why is there localisation of disease to 1st molars and incisors in LAP?
Often subjects present with attachment loss that does not fit the specific diagnostic criteria (AP or chronic periodontitis).
Schenkein et al. 1995: cigarette smoking was shown to be a risk factor for patients with generalized forms of AgP.
Smokers with GAP had more affected teeth and greater mean levels of attachment loss than patients with GAP who did not smoke.
IgG2 serum levels as well as antibody levels against A.a. are significantly depressed in subjects with GAP who smoked.
Periodontitis is a complex infection initiated by bacteria –tissue destruction.
Host: the organism from which a parasite obtains its nourishment/ an individual who receives a graft
Modulation: the alteration of function or status of something in response to a stimulus or an altered physical or chemical environment
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.
Malocclusion is the misalignment of teeth and jaws, or more simply, a "bad bite". Malocclusion can cause a number of health and dental problems.
Static occlusion refers to contact between teeth when the jaw is closed and stationary, while dynamic occlusion refers to occlusal contacts made when the jaw is moving. Dynamic occlusion is also termed as articulation. During chewing, there is no tooth contact between the teeth on the chewing side of the mouth.
Centric occlusion is the occlusion of opposing teeth when the mandible is in centric relation. Centric occlusion is the first tooth contact and may or may not coincide with maximum intercuspation. It is also referred to as a person's habitual bite, bite of convenience, or intercuspation position (ICP). Centric relation, not to be confused with centric occlusion, is a relationship between the maxilla and mandible. Dr Harshavardhan Patwal , Malocclusion is the result of the body trying to optimize its function in a dysfunctional environment. It can be associated with a number of problems, including crooked teeth, gum problems, the temporomandibular joint (TMJ), and jaw muscles. Teeth, fillings, and crowns may wear, break, or loosen, and teeth may be tender or ache. Receding gums can be exacerbated by a faulty bite. If the jaw is mispositioned, jaw muscles may have to work harder, which can lead to fatigue and or muscle spasms. This in turn can lead to headaches or migraines, eye or sinus pain, and pain in the neck, shoulder, or even back. Malocclusion can be a contributing factor to sleep disordered breathing which may include snoring, upper airway resistance syndrome, and / or sleep apnea (apnea means without breath). Untreated damaging malocclusion can lead to occlusal trauma.
Some of the treatments for different occlusal problems include protecting the teeth with dental splints (orthotics), tooth adjustments, replacement of teeth, medication (usually temporary), a diet of softer foods, TENS to relax tensed muscles, and relaxation therapy for stress-related clenching. Removable dental appliances may be used to alter the development of the jaws. Fixed appliances such as braces may be used to move the teeth in the jaws. Jaw surgery is also used to correct malocclusion.
Certains medications have been associated with gingival enlargement.
the seminar gives a complete analysis of etilogy and pathogenesis involved in digo as well as sequlae of it
Periodontal risk & making risk assessmentibrahimaziz15
Periodontal risk and risk assessment is very importnant in monitoring periodontally affected patients, this seminar will give you an idea about periodontal risk factors and how to make a periodontal risk assessment for patients.
Systemic Peridoontology, link between systemic health and periodontology, diabetes and periodontology, Pregnancy and Peridotology,Nutrition and periodontology
AGGRESSIVE PERIODONTITIS
PRESENTER
DR. REBICCA RANJIT
DEPT. OF PERIODONTOLOGY & ORAL IMPLANTOLOGY
Why is there localisation of disease to 1st molars and incisors in LAP?
Often subjects present with attachment loss that does not fit the specific diagnostic criteria (AP or chronic periodontitis).
Schenkein et al. 1995: cigarette smoking was shown to be a risk factor for patients with generalized forms of AgP.
Smokers with GAP had more affected teeth and greater mean levels of attachment loss than patients with GAP who did not smoke.
IgG2 serum levels as well as antibody levels against A.a. are significantly depressed in subjects with GAP who smoked.
Periodontitis is a complex infection initiated by bacteria –tissue destruction.
Host: the organism from which a parasite obtains its nourishment/ an individual who receives a graft
Modulation: the alteration of function or status of something in response to a stimulus or an altered physical or chemical environment
Occlusion, in a dental context, means simply the contact between teeth. More technically, it is the relationship between the maxillary (upper) and mandibular (lower) teeth when they approach each other, as occurs during chewing or at rest.
Malocclusion is the misalignment of teeth and jaws, or more simply, a "bad bite". Malocclusion can cause a number of health and dental problems.
Static occlusion refers to contact between teeth when the jaw is closed and stationary, while dynamic occlusion refers to occlusal contacts made when the jaw is moving. Dynamic occlusion is also termed as articulation. During chewing, there is no tooth contact between the teeth on the chewing side of the mouth.
Centric occlusion is the occlusion of opposing teeth when the mandible is in centric relation. Centric occlusion is the first tooth contact and may or may not coincide with maximum intercuspation. It is also referred to as a person's habitual bite, bite of convenience, or intercuspation position (ICP). Centric relation, not to be confused with centric occlusion, is a relationship between the maxilla and mandible. Dr Harshavardhan Patwal , Malocclusion is the result of the body trying to optimize its function in a dysfunctional environment. It can be associated with a number of problems, including crooked teeth, gum problems, the temporomandibular joint (TMJ), and jaw muscles. Teeth, fillings, and crowns may wear, break, or loosen, and teeth may be tender or ache. Receding gums can be exacerbated by a faulty bite. If the jaw is mispositioned, jaw muscles may have to work harder, which can lead to fatigue and or muscle spasms. This in turn can lead to headaches or migraines, eye or sinus pain, and pain in the neck, shoulder, or even back. Malocclusion can be a contributing factor to sleep disordered breathing which may include snoring, upper airway resistance syndrome, and / or sleep apnea (apnea means without breath). Untreated damaging malocclusion can lead to occlusal trauma.
Some of the treatments for different occlusal problems include protecting the teeth with dental splints (orthotics), tooth adjustments, replacement of teeth, medication (usually temporary), a diet of softer foods, TENS to relax tensed muscles, and relaxation therapy for stress-related clenching. Removable dental appliances may be used to alter the development of the jaws. Fixed appliances such as braces may be used to move the teeth in the jaws. Jaw surgery is also used to correct malocclusion.
Dr. Rahul VC Tiwari - Fellowship In Orthognathic Surgery - Jubilee Mission Medical College Hospital and Research Center, Thrissur, Kerala - 31st publication IJAR 1st name
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
3. AAOMFS Definition in 2022 Update
Current or previous treatment with antiresorptive therapy alone or in combination with
immune modulators or antiangiogenic medications.
Exposed bone or bone that can be probed through an intraoral or extra-oral fistula(e)
in the maxillofacial region that has persisted for more than eight weeks.
No history of radiation therapy to the jaws or metastatic disease to the jaws.
Anatomic Factors:
Mandible 75%
Maxilla 25%
Both Jaws 4.5%
4. Predisposing Factors
Dentoalveolar Surgery; the most common identifiable predisposing factor for
developing MRONJ 62-82%
Concomitant Oral Disease; a risk factor among 50 percent of the cases.
Trauma
Smoking
Steroids,
Immunocompromised host
Autoimmune diseases
Diabetes
Chemotherapy.
11. C-Terminal Telopeptide Test (CTX)
Female (premenopausal): 40-465 pg/mL.
Female (postmenopausal): 104-1008 pg/mL.
Male: 60-700 pg/mL.
Elevated levels are found in osteoporosis patients with elevated bone turnover who are
at increased risk for rapid disease progression.
Increased levels are also associated with osteopenia, Paget disease of the bone,
hyperthyroidism, and hypothyroidism.
12. C-Terminal Telopeptide Test
The risk of MRONJ following a dental procedure in patients on bisphosphonates was
High if the CTX level was below 100 pg/ml
Moderate at 100–150 pg/ml
Low above 150 pg/ml
15. Different Names
ARONJ; Anti-Resorptive -induced osteonecrosis of the jaws.
DIRONJ; drug-induced osteonecrosis of the jaws.
MRONJ; medication-induced osteonecrosis of the jaws.
Zoledronic acid, the most potent bisphosphonate.
16. Bisphosphonates
Antiresorptive medications that are effective in managing cancer-related conditions
Including hypercalcemia of malignancy, spinal cord compression and pathologic
fractures associated with bone metastases in the context of solid tumors (such as
breast, prostate and lung cancers) and multiple myeloma.
Used for the prevention of osteoporosis-related fractures (fragility fractures)
BPs administered:
Orally including alendronate (Fosamax), risedronate (Actonel)
Parenterally (zoledronic acid [Reclast]), and ibandronate (Boniva)
Can result in a significant reduction in vertebral and non-vertebral fractures for patients
with osteoporosis
17. Definition
Bisphosphonates Work by:
1. Inhibition of osteoclast recruitment
2. Reduction of osteoclast life span
3. Inhibition of osteoclastic activity at the bone surface.
Bisphosphonate medications can also be used to treat Paget’s disease of bone and
osteogenesis imperfecta.
Bisphosphonates inhibit osteoclast activity and prevent bone breakdown.
Bisphosphonates also affect osteoblast activity, secondarily affects osteoclast activity.
The half-life of this medication is long, measured in years.
18. Patients About to Initiate Bisphosphonate Therapy
The goal in this group is to prevent the development of ONJ.
If at all possible, the initiation of bisphosphonate therapy should be delayed until
oral/dental health is optimized.
Non-restorable teeth and teeth with poor prognoses should be extracted.
It is recommended to allow 14–21 days to allow adequate healing before starting
bisphosphonate therapy. [2 months American Guidelines]
Restorative dentistry, scaling, and prophylaxis are best completed before initiation of
bisphosphonate therapy.
Patients should be educated about the importance of good oral and dental hygiene.
Routine dental examinations and evaluations are important to monitor patient
compliance and to detect problems early rather than at a later stage.
19. Patients Receiving Bisphosphonate Therapy
Patients should maintain good oral and dental hygiene in order to prevent problems
that require osseous surgery.
Dental procedures that involve bony surgery should be avoided.
Endodontic therapy is preferable to extraction of teeth.
Placement of dental implants should be avoided.
The incidence of developing ONJ in patients receiving intravenous bisphosphonates is
higher than in patients receiving oral bisphosphonate therapy
22. Patients Receiving Oral Bisphosphonates
The risk of ONJ appears to be associated with a longer duration of therapy, 3 years or
greater.
In patients who have taken oral bisphosphonates for less than 4 years and have no
clinical risk factors, no alteration in the planned dento-alveolar treatment is required.
Risk factors include conditions that may adversely affect healing, such as steroid
treatment, diabetes and other medications, and medical conditions that would make
the patient immunocompromised.
In patients who have taken oral bisphosphonates for less than 4 years but have clinical
risk factors, a “drug holiday” of at least 2 months should be considered before
Dentoalveolar surgery.
23. Drug Holiday
A pre-operative drug holiday of 3–6 months has been recommended for patients with a
3-year or greater history of bisphosphonate use
27. In patients who have taken oral bisphosphonates for greater than 4 years (with or
without risk factors), a drug holiday of 2 months should be considered before
dentoalveolar surgery.
Drug Holiday:
Pre-Op: 2 months (American Guidelines)
Pre-Op: 3-6 months (European and German)
Post-op: 2 months (American Guidelines)
Post-Op: 3-6 months (European and German)
A total period of 6-9 months
Patients Receiving Oral Bisphosphonates
28.
29. Staging
Patients at-Risk
No apparent necrotic bone in asymptomatic patients who have been treated with IV or
oral antiresorptive therapy.
30. Staging
Stage 0
Patients with no clinical evidence of necrotic bone
Nonspecific clinical and radiographic findings
Pain and change in the bony trabecular pattern of the jaws; Dull, aching bone pain in
the jaw, which may radiate to the temporomandibular joint region.
Progression to Stage 1 disease has been reported in up to 50 percent of patients with
Stage 0 disease.
Treatment Strategy
Clinical follow-up is recommended with conservative treatment.
Clinicians should provide symptomatic treatment such as pain control and
manage any treatable condition such as dental caries and periodontal disease
31. Staging
Stage 1; Patients have exposed and necrotic bone.
Asymptomatic
No sign of infection.
Treatment Strategy
Oral anti-microbial rinses; chlorhexidine 0.12%, are indicated.
Close monitoring of the oral condition and maintaining good oral hygiene are
recommended.
Surgical treatment is generally not recommended.
Sharp bony edges that are irritating oral tissues may be smoothed down.
32. Staging
Stage 2: Patients have exposed and necrotic bone
Symptomatic with pain and infection.
Treatment Strategy
Oral antimicrobial rinses are recommended in conjunction with antibiotic
therapy.
Penicillin is still effective in the management of MRONJ with infection.
Quinolones, metronidazole, clindamycin, doxycycline, and erythromycin have
been used empirically in penicillin-allergic patients.
Refractory cases may require intravenous antibiotic treatment along with
maintenance of suppressive treatment to manage the disease.
33. Staging
Stage 3
Patients have exposed and necrotic bone
Symptomatic with pain and infection and one or more of the following:
Exposed and necrotic bone extending beyond the alveolar bone.
Pathologic fracture.
Extraoral fistula.
Oral-antral or oral-nasal communication.
Osteolysis extending to the inferior border of the mandible or maxillary sinus floor.
34. Staging – Stage 3 Management
Surgical debridement, including resection, is used in conjunction with antibiotic
treatment.
Resection is generally reserved for extensive, late presentation of disease and
pathologic fractures
Mobile segments of bony sequestrum should be removed regardless of the disease
stage.
Care should be taken not to expose the uninvolved bone for fear of extending the
disease process.
Stopping intravenous bisphosphonates appears to offer no short-term benefit.
Long-term cessation of bisphosphonate therapy may be beneficial in patient healing
35. Long-Term Follow-up
Long-term patients were noted to have spontaneous fractures in their long bones,
specifically the femur.
Long term is felt to be greater than 5 years but some fractures occurred after 2 years
of oral bisphosphonate therapy.
These fractures occurred with walking and low-energy injuries.
This has caused clinicians to reevaluate their recommendations for stopping oral
bisphosphonate medications for a period of time(drug holiday) and allow the bone to
resume a more normal state of resorption and deposition.
The final therapeutic regimen of oral bisphosphonate therapy has yet to be
determined.
52. Definition
Inflammation of the bone marrow with a tendency to progression.
It involves the adjacent cortical plates and periosteal tissues.
The incidence of osteomyelitis is higher in the mandible due to the dense, poorly
vascularized cortical plates and blood supply primarily from the inferior alveolar
neurovascular bundle, a single source.
Osteomyelitis is less common in the maxilla due to the excellent blood supply from
multiple feeder vessels and less bone density.
53. Local and Systemic Factors
Diabetes
Autoimmune states
Malignancy, malnutrition,
Acquired immunodeficiency syndrome (AIDS).
Medications such as steroids and chemotherapeutic agents.
Local conditions; Osteopetrosis, bone pathology, and repeated surgeries can alter the
blood supply to the area.
54. Pathogenesis
Osteomyelitis primarily occurs as a result of contiguous spread of odontogenic infections,
Dentoalveolar surgery and maxillofacial trauma.
Any Dentoalveolar surgical procedure can potentially cause an osteomyelitis.
The initial insult results in a bacteria- induced inflammatory process.
In the normal healthy host, this process is self-limiting and is a component of the healing
process
With inflammation there is hyperemia and increased blood flow to the affected area
Pus is formed when there is an overwhelming abundance of bacteria and cellular debris
that cannot be eliminated by the body’s natural defense mechanisms.
When the pus and subsequent inflammatory response occur in the bone marrow, an
elevated intramedullary pressure is created which further decreases the blood supply to
the area.
55. Pathogenesis
Pus can travel via Haversian and Volkmann’s canals to spread throughout the
medullary and cortical bone.
Once pus has perforated the cortical plates and collects under the periosteum, the
periosteal blood supply is compromised.
Intra-oral or Extra-oral Fistula
56. Microbiology
The major pathogenic species are streptococci and anaerobic bacteria; Staphylococcal
species.
The anaerobes responsible are generally bacteroides or peptostreptococci species.
Often the infections are mixed species, growing several oral pathogens on final
culture.
Penicillin and metronidazole as dual drug therapy or clindamycin or Unasyn
(ampicillin/sulbactam)
Viral osteomyelitis has been reported
57. Classification
Currently, there is no universally accepted classification system for osteomyelitis.
Suppurative or Non-Suppurative by Lew and Waldvogel.
Hematogenous or secondary to a contiguous focus of infection.
Acute or Chronic by Hudson; the most advantageous
Osteomyelitis is classified into acute and chronic forms based on the presence of the
disease for a 1-month duration.
61. Laboratory Investigations
Complete Blood Count with Differential
C-Reactive Protein; Not Specific
Erythrocyte Sedimentation Rate; Not Specific
Radiographic Examination:
OPG; Moth-Eaten Appearance
CT; Gold Standard, requires 30–50% demineralization of bone before changes can be
seen
MRI; Early Stage of Osteomyelitis by loss of marrow signal before sequestration
Nuclear Imaging; T-99 is very sensitive to areas of High turnover
The addition of Gallium 67 or indium 111 as contrast agents, one can differentiate
areas of infection from trauma or postsurgical healing.
62. Three-Phase T-99 Imaging Study
The technologist starts imaging and injects the patient.
Images are obtained at 1 to 3 seconds per frame (when using digital images) for a
video clip lasting 60 seconds which is referred to as "dynamic imaging."
This dynamic imaging demonstrates and characterizes relative perfusion to a particular
area and is called the "flow phase" or "angiographic phase."
Following this step, a second image is obtained in the same field of view and is termed
the "blood pool" phase.
This characterizes blood pool accumulation in the soft tissues and bone (or lack
thereof) as a result of flow and capillary dilatation.
Two to 3 hours after initial injection, the third phase, termed "delayed," includes images
of the same location as the earlier phases and will also include either the whole body
or the lower half of the body.
63. Terms
A sequestrum is a segment of necrotic bone that becomes separated or “sequestered”
from the healthy intact bone.
The reactive bone that forms around the necrotic sequestrum is referred to as
the Involucrum
The draining tract extending from the skin to the sequestrum is termed the
cloaca.
67. Treatment
Both medical and surgical interventions.
In rare cases of infantile osteomyelitis, intravenous antibiotic therapy alone may
eradicate the disease.
Correct Diagnosis and Medical Evaluation
Empiric antibiotic treatment should be started based on Gram stain results of the
exudate.
Definitive culture and sensitivity reports generally take several days or longer to be
obtained.
68. Surgical Options
Classic treatment is sequestrectomy and saucerization.
The aim is to debride the necrotic or poorly vascularized bony sequestrum in the
infected area and improve blood flow.
Sequestrectomy involves removing infected and avascular pieces of bone
Saucerization involves the removal of the adjacent bony cortices and open packing to
permit healing by secondary intention.
Decortication involves removal of the dense, often chronically infected and poorly
vascularized bony cortex.
It is often necessary to remove teeth adjacent to an area of osteomyelitis.
69. Surgical Options
Fixation device (external fixator or reconstruction type plate) and/or placing the patient
in maxilla-mandibular fixation is frequently used to prevent pathologic fracture.
Some authors proposed adjunctive treatment therapy that deliver high doses of
antibiotic to the area using antibiotic impregnated beads or wound irrigation systems.
This therapy works on high local levels of antibiotics; the overall systemic load is very
low, thus reducing the possible side effect and complication rate.
Hyperbaric oxygen (HBO) treatment has also been advocated for the treatment of
refractory osteomyelitis.
HBO works on increasing tissue oxygenation levels that would help fight off any
anaerobic bacteria present in these wounds
70. Surgical Options
Resection of the jaw bone has traditionally been reserved as a last-ditch effort,
generally after smaller debridement procedures have been performed or previous
therapy has been unsuccessful or to remove areas involved with pathologic fracture.
This resection is generally performed via an extra-oral route, and reconstruction can
be either immediate or delayed based on the surgeon’s preference.
Rigid internal fixation has simplified the postoperative course by providing a means for
immediate function of the jaws.
The custom milled plates are very precise and require little or no additional bending.
The custom milled plates are stronger than traditional plates and are less prone to
fracture.
Inferior alveolar nerve preservation and immediate reconstructive surgery with bone
grafts have shortened the clinical course for our patients
77. Question 1: MRONJ is more common in:
A) Maxilla
B) Mandible
C) Both Jaws
D) Other Bones in the human body
78. Question 2
A female patient presented to your practice complaining of Pain due to a badly
decayed wisdom tooth, after history taking the patient has osteoporosis and she takes
oral bisphosphonates for less than 4 years and with no clinical risk factors, extraction
is planned for this Patient, which of the following statements is true regarding the
planned procedure:
A) Extraction is contraindicated in this case due to high risk of MRONJ
B) No alteration in the planned dento-alveolar treatment is required.
C) Prescribe Antibiotics and Analgesics and Defer the patient
D) All of the above can be considered