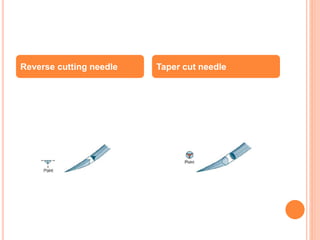
This document describes various materials and methods used for surgical wound closure and anastomoses. It discusses suture materials including absorbable and non-absorbable synthetic and natural options. It also covers other closure methods like staples, tissue glue, and skin adhesive strips. The document details types of sutures, needles, and common knotting techniques used to accurately approximate tissue edges during surgery.