Downloaded 141 times
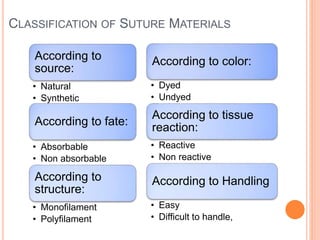
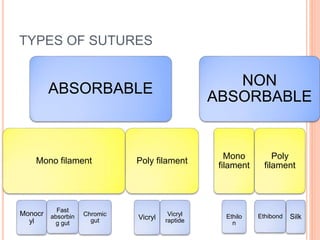
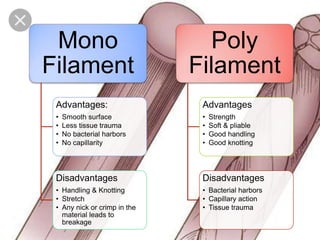
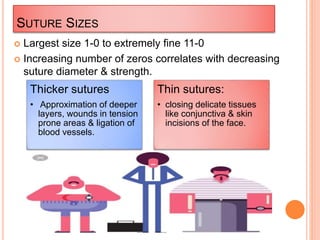



This document provides an overview of principles of suturing in surgery. It defines what a suture is, the goals of suturing, types of suture materials and their classifications. It also describes suture sizes, needles, principles of suture selection and different suturing techniques. Interrupted, continuous, mattress and figure-of-eight sutures are explained. Knot tying, suture removal and potential complications are also summarized. The document serves as a comprehensive guide to suturing in surgical procedures.

















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





