The document discusses concepts related to sepsis, severe sepsis, and septic shock. It provides statistics on the incidence and mortality of these conditions. It also describes the pathophysiology of sepsis, including the roles of inflammation, coagulation abnormalities, and hemodynamic changes. Potential mediators such as cytokines, nitric oxide, and endotoxin are examined in the development of septic shock.
Overview of sepsis and septic shock by Anand Kumar, MD, presenting concepts from the University of Manitoba.
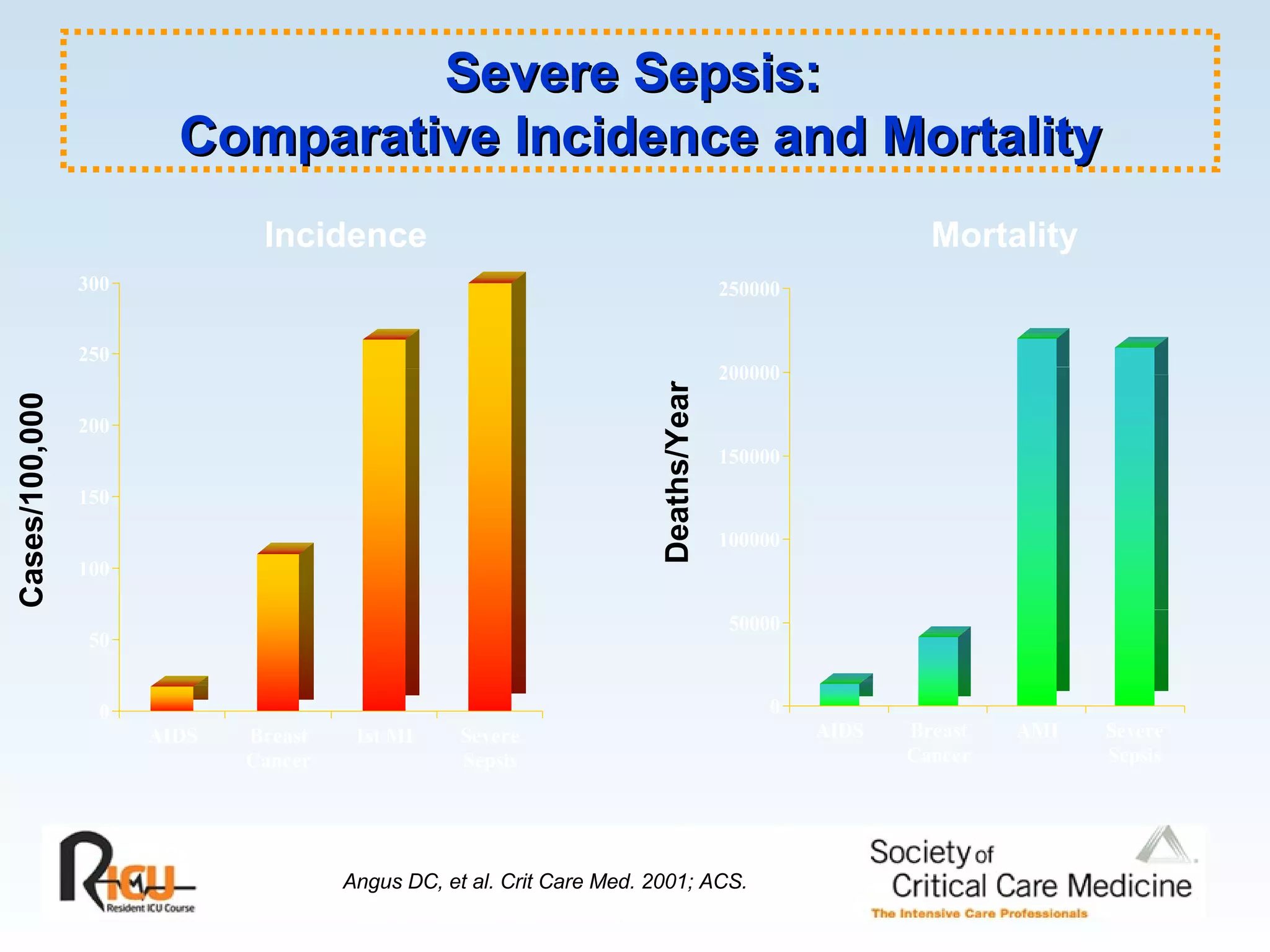
Annual incidence (800,000 severe sepsis; 400,000 septic shock) with death rates (35-50% mortality). Data shows unchanged mortality rates even post-antibiotics.
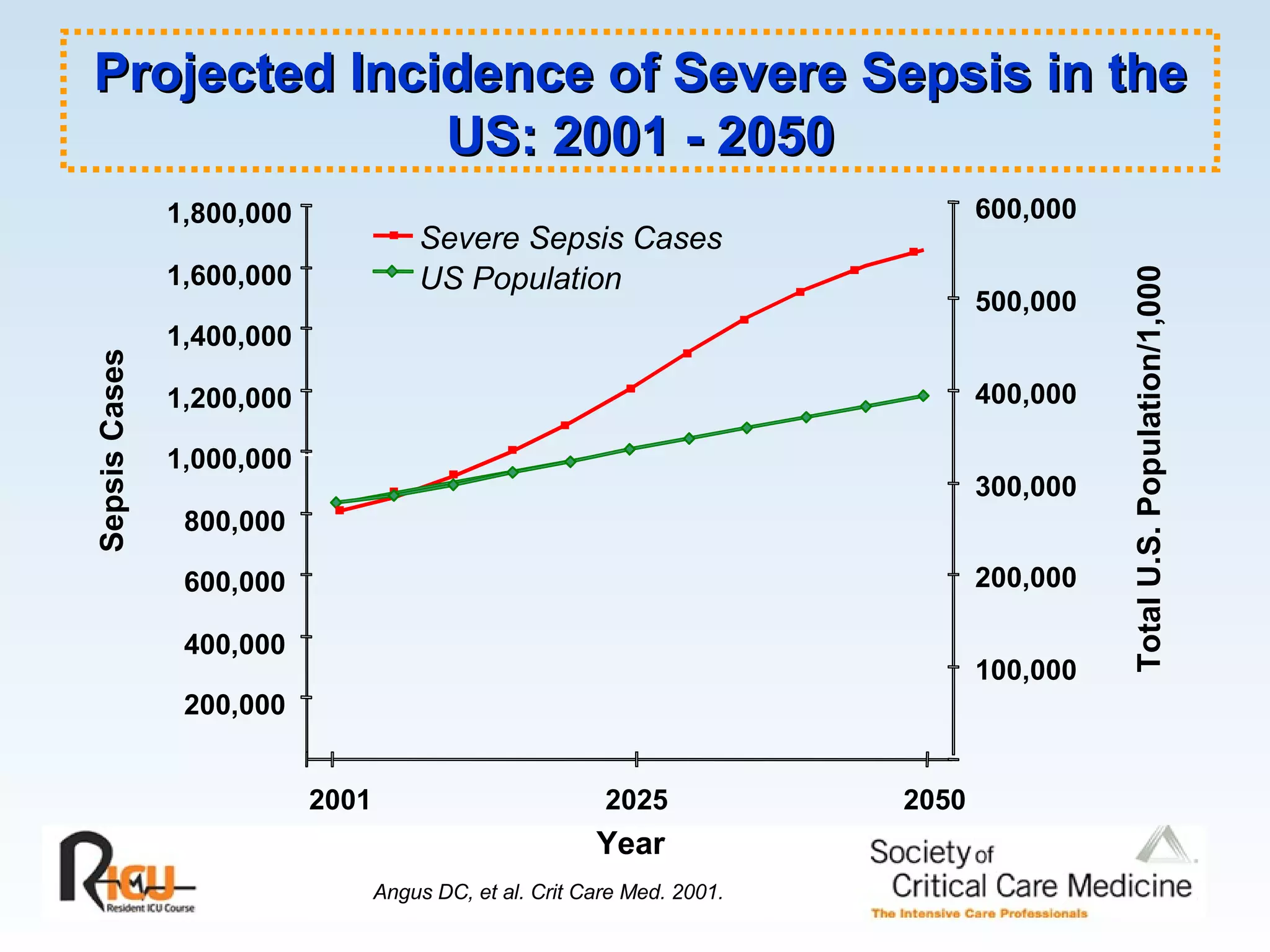
Projected increase in severe sepsis cases in the USA from 2001 to 2050, predicting as much as 1,600,000 cases.
Definitions of SIRS, sepsis, severe sepsis, and septic shock with criteria for evaluation of each condition.
Understanding the relationships among sepsis, severe sepsis, and septic shock including comorbidities.
In-depth views on sources of infection, toxins involved in pathogenesis, and organ dysfunction mechanisms.
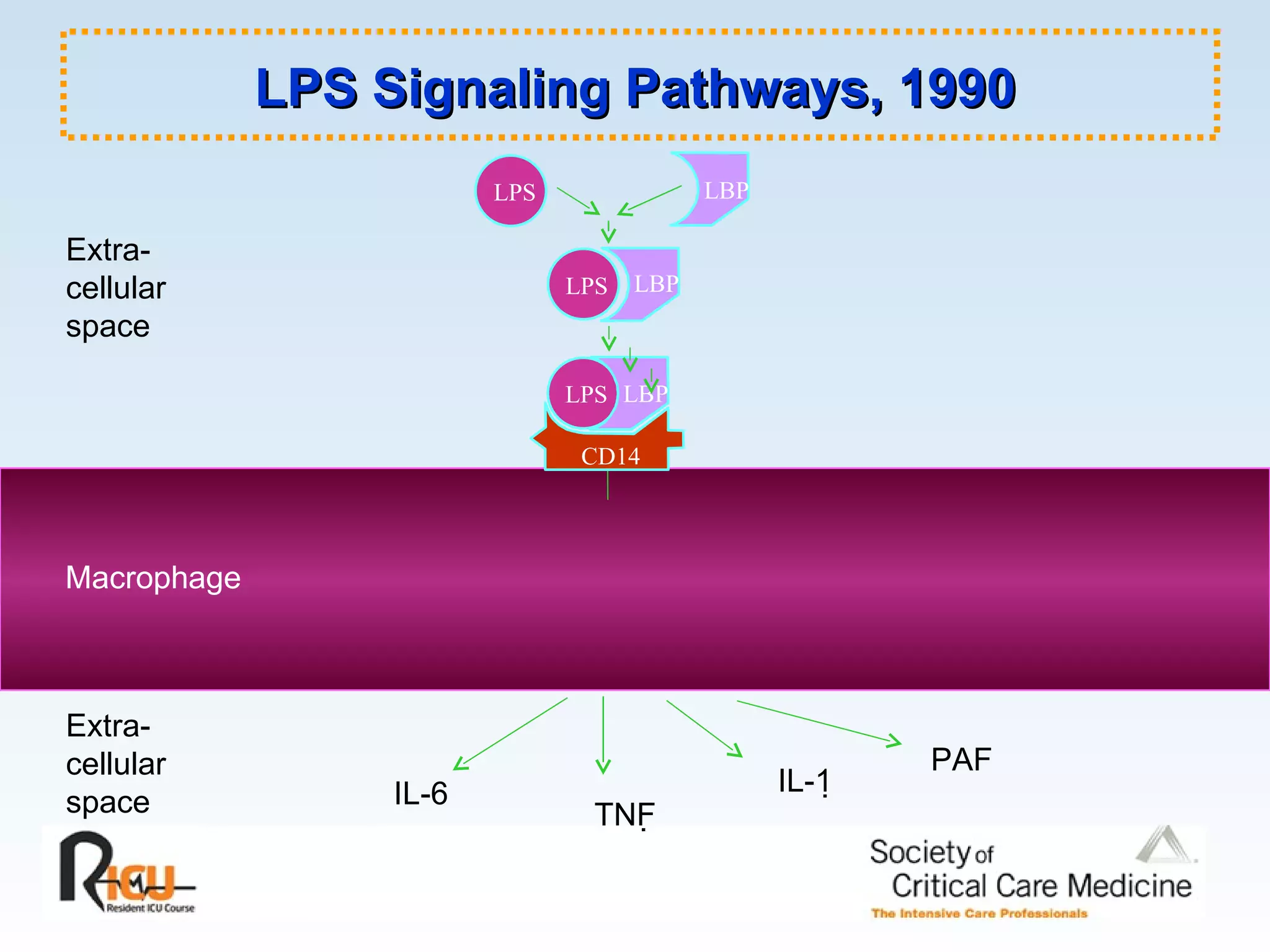
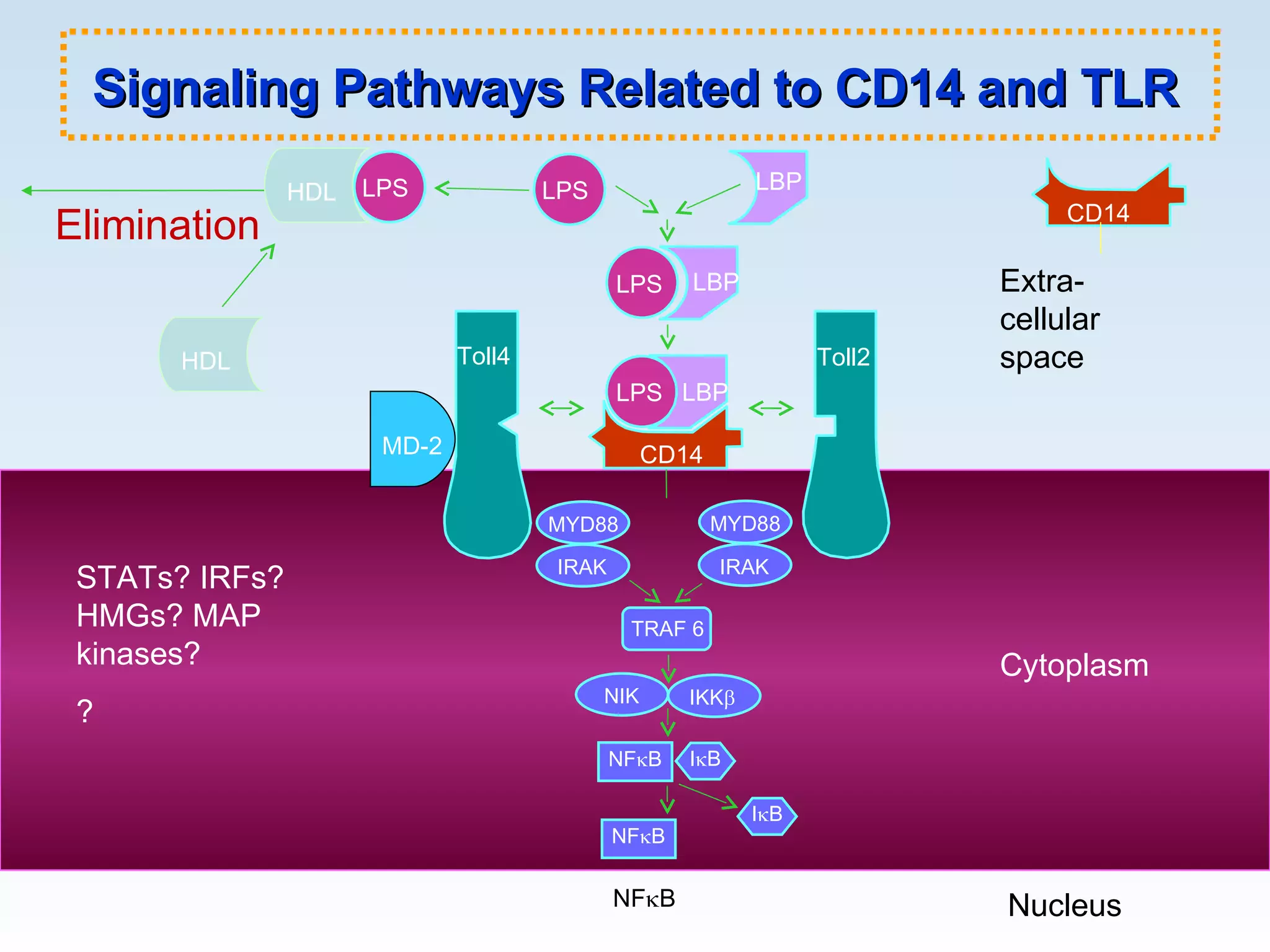
Cytokine pathways involved, endothelial dysfunction, and cellular signaling related to septic shock and its effects.
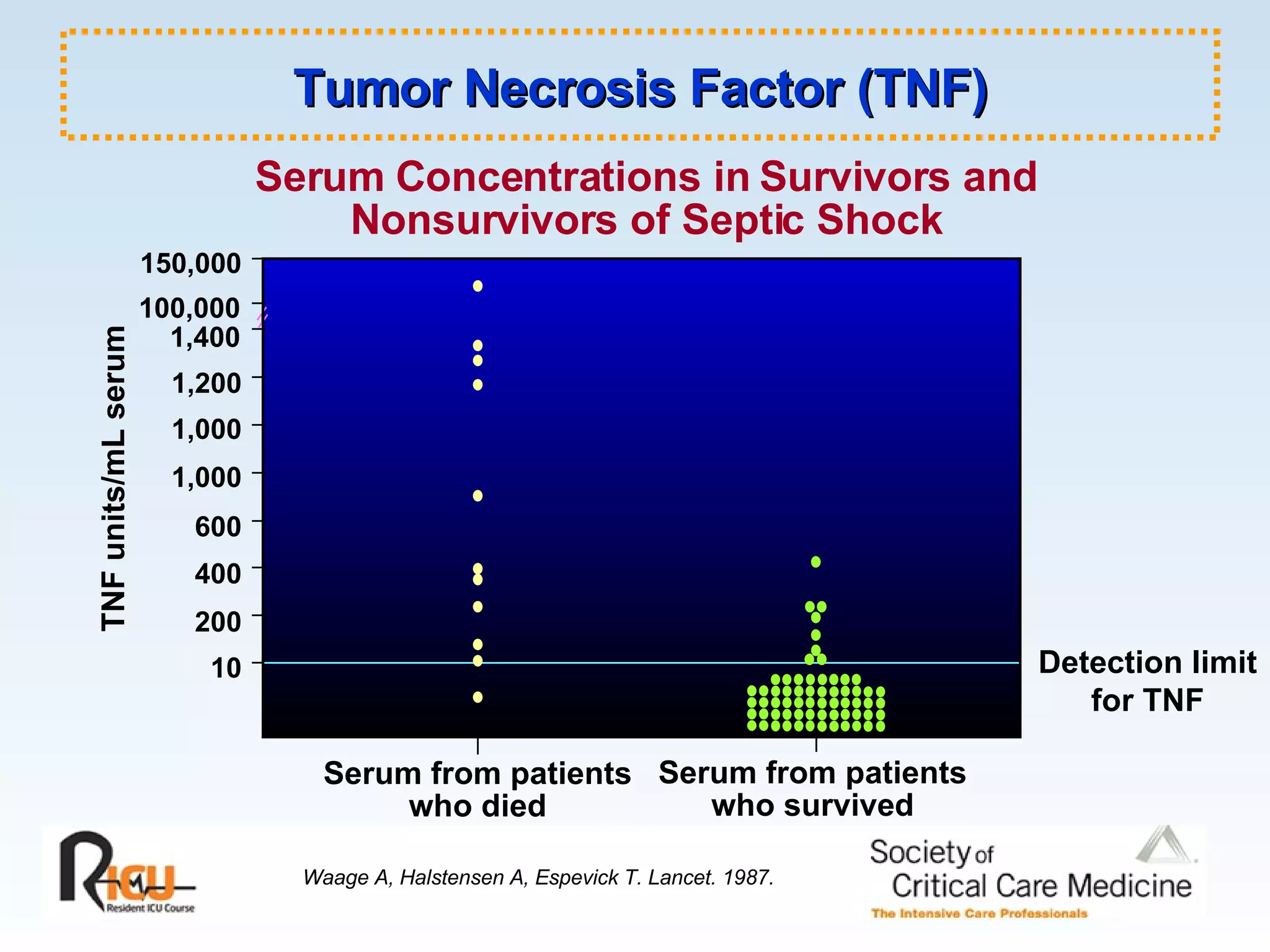
Fluid changes in septic patients indicating cytokines like TNF, their levels in survivors vs nonsurvivors.
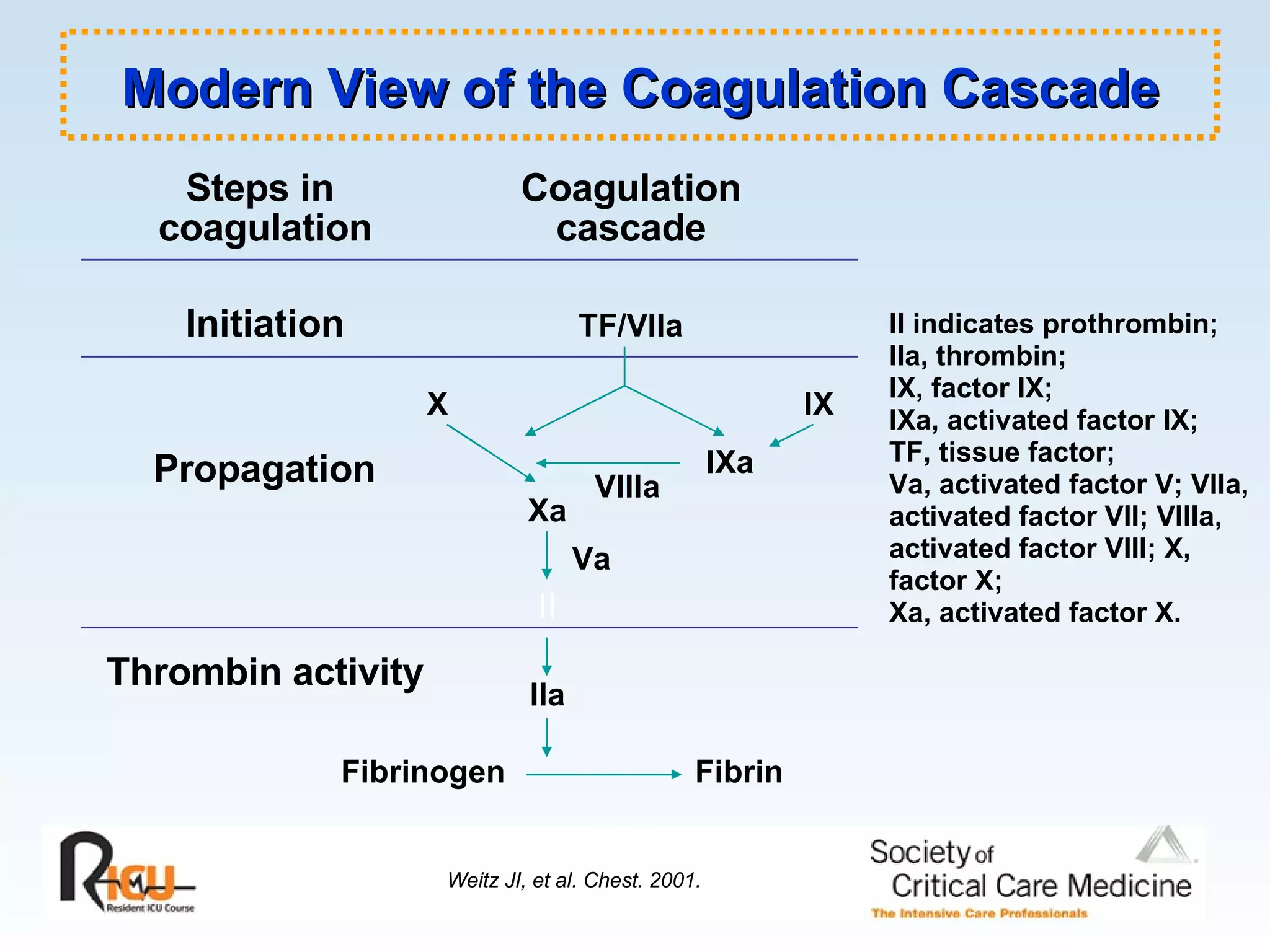
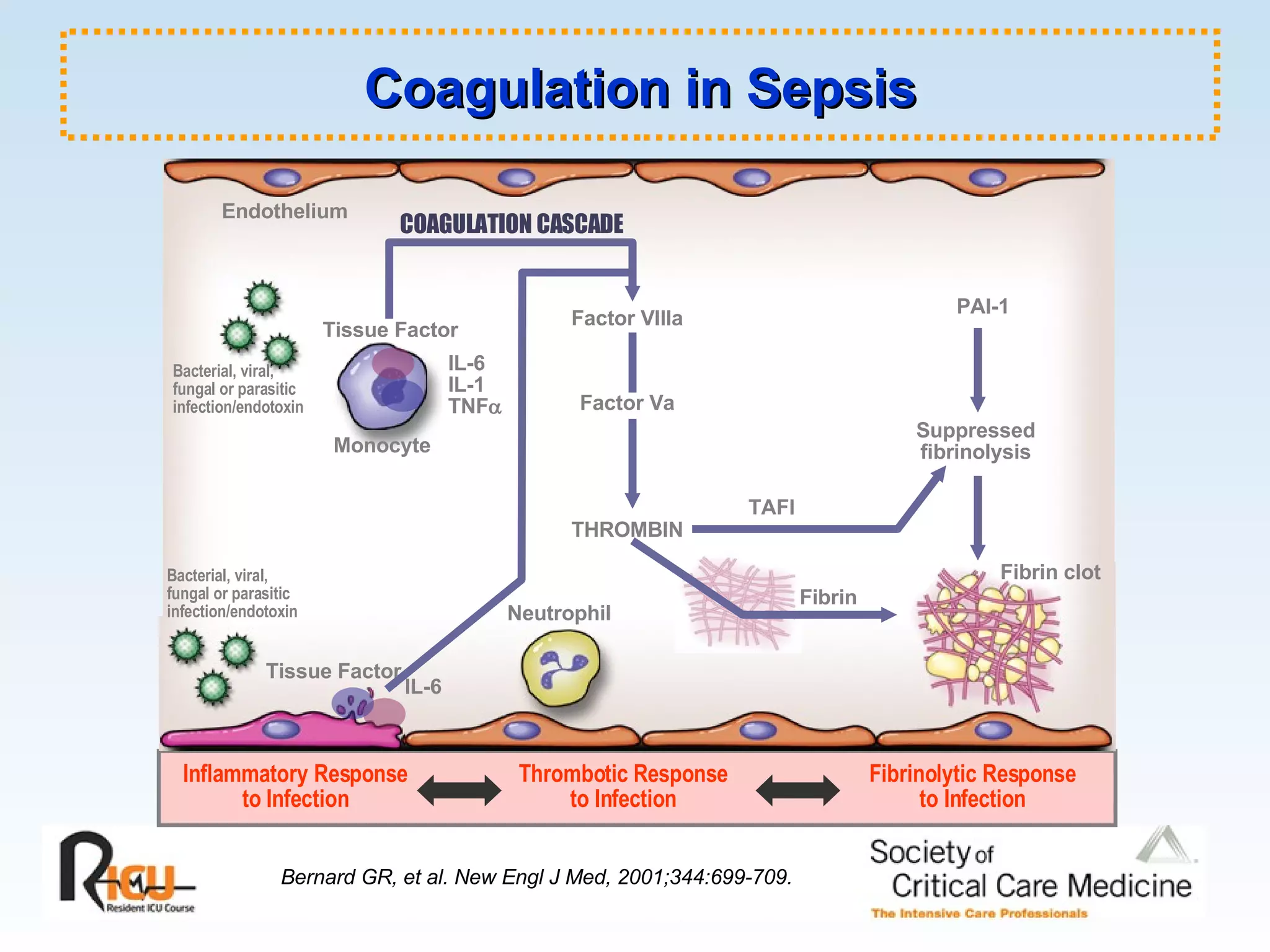
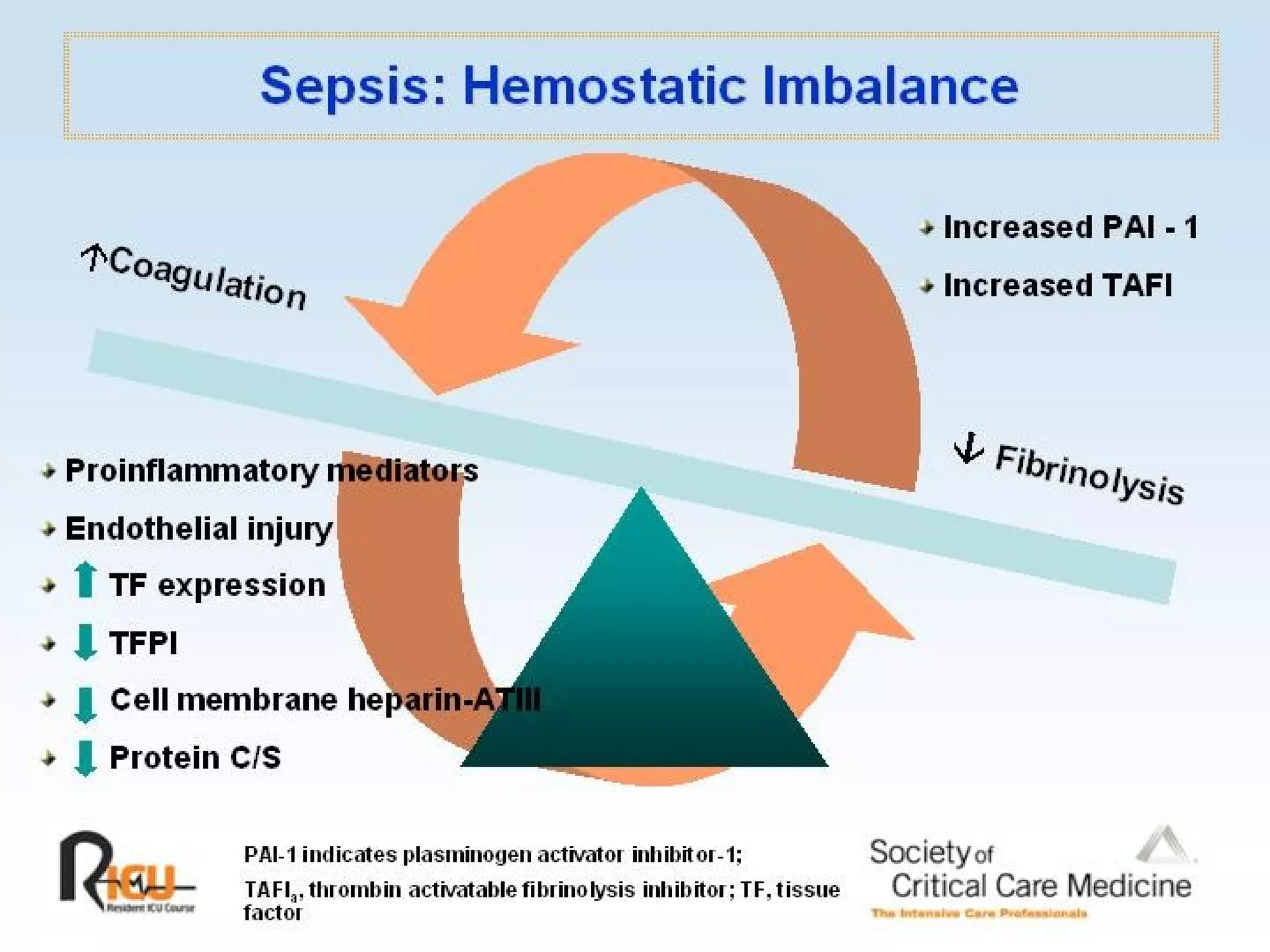
Pathophysiology of sepsis highlighting coagulation cascade and markers of coagulopathy and sepsis diagnosis.
Role of nitric oxide in vascular responses and its impact during septic conditions.
Analysis of hemodynamic states including warm and cold shock, and oxygen delivery relationship in septic shock.
Explores metabolic derangements in sepsis alongside references for further reading and significant studies.
Section of CriticalCare Medicine Section of Infectious Diseases University of Manitoba, Winnipeg, Canada UMDNJ-Robert Wood Johnson Medical School Cooper Hospital, NJ Anand Kumar, MD Sepsis and Septic Shock Old Concepts, New Precepts
2.
Incidence of SevereSepsis/Septic Shock Approximate Cases/Year 800,000 600,000 400,000 200,000 0 Severe sepsis 800,000 Septic shock 400,000 Deaths from septic shock 200,000 Sepsis and sequelae are a leading cause of death in ICU Mortality in septic shock remains at 35 - 50% -unchanged since advent of antibiotics (from 55 - 75%)
3.
Bacterial Sepsis DeathRate in the United States 5.0 Chart adapted from CDC/National Center for Health Statistics, 1992. 4.0 3.0 2.0 1.0 0.0 0.8 0.7 0.5 0.4 0.6 0.2 0.1 0.3 1960 1965 1970 1975 1980 1985 1990 Rate per 100,000 Population 4.1
4.
Severe Sepsis: Comparative Incidence and Mortality Angus DC, et al. Crit Care Med. 2001; ACS. Incidence Cases/100,000 Mortality Deaths/Year
5.
Mortality of SevereSepsis by Age in the United States Angus DC, et al. Crit Care Med. 2001. 0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 0 1 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 Age Mortality Without Co-morbidity With Co-morbidity Overall
6.
Projected Incidence ofSevere Sepsis in the US: 2001 - 2050 200,000 400,000 600,000 800,000 1,000,000 1,200,000 1,400,000 1,600,000 1,800,000 2001 2025 2050 Year 100,000 200,000 300,000 400,000 500,000 600,000 Severe Sepsis Cases US Population Sepsis Cases Total U.S. Population/1,000 Angus DC, et al. Crit Care Med. 2001.
7.
Systemic Inflammatory ResponseSyndrome (SIRS) Systemic inflammatory response to a variety of severe clinical insults. Manifested by two or more of the following: Temperature > 38 o C or < 36 o C Heart rate > 90 beats/min Respiratory rate > 20 breaths/min or PaCO 2 < 32 mm Hg WBC > 12,000/mm 3 , < 4000/mm 3 , or > 10% immature (band) forms ACCP/SCCM Consensus Statement Chest. 1992;1644-1655.
8.
Sepsis: ACCP/SCCM DefinitionsInfection Inflammatory response to microorganisms or invasion of normally sterile tissues Sepsis The systemic response to infection – i.e., confirmed or suspected infection plus 2 SIRS criteria Severe Sepsis Sepsis associated with organ dysfunction, hypoperfusion, or hypotension Hypoperfusion abnormalities may include but are not limited to lactic acidosis, oliguria, acute alteration in mental status ACCP/SCCM Consensus Statement. Chest. 1992;101:1644-55.
9.
Sepsis - ACCP/SCCMDefinitions: The Update Altered mental status Edema or increased fluid balance Hyperglycemia (absent diabetes) Increased CRP or procalcitonin Hypotension Increased SvO 2 CI > 3.5 L/min/m 2 Arterial hypoxemia (PaO 2 /FiO 2 < 300) Acute oliguria (> 2 hours) Increased serum Cr (> 0.5 mg/dL) Coagulopathy (INR > 1.5) Ileus (absent bowel sounds) Thrombocytopenia (< 100,000/uL) Hyperbilirubinemia (> 40 mg/dL or 70 mmol/L) Hyperlactatemia (> 1 mmol/L) Decreased capillary refill or mottling Levy MM, et al. Crit Care Med. 2003.
10.
Septic Shock :ACCP/SCCM Definition Sepsis-induced hypotension despite adequate fluid resuscitation along with the presence of perfusion abnormalities that may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration of mental status; patients receiving inotropic or vasopressor agents may not be hypotensive at the time that perfusion abnormalities are measured. ACCP/SCCM Consensus Statement. Chest. 1992;101:1644-55.
11.
12.
13.
Relationship of Sepsis,Severe Sepsis, and Septic Shock Sepsis Severe Sepsis Septic shock MODS Death Sepsis and organ dysfunction, hypoperfusion, or hypotension Sepsis-induced hypotension
14.
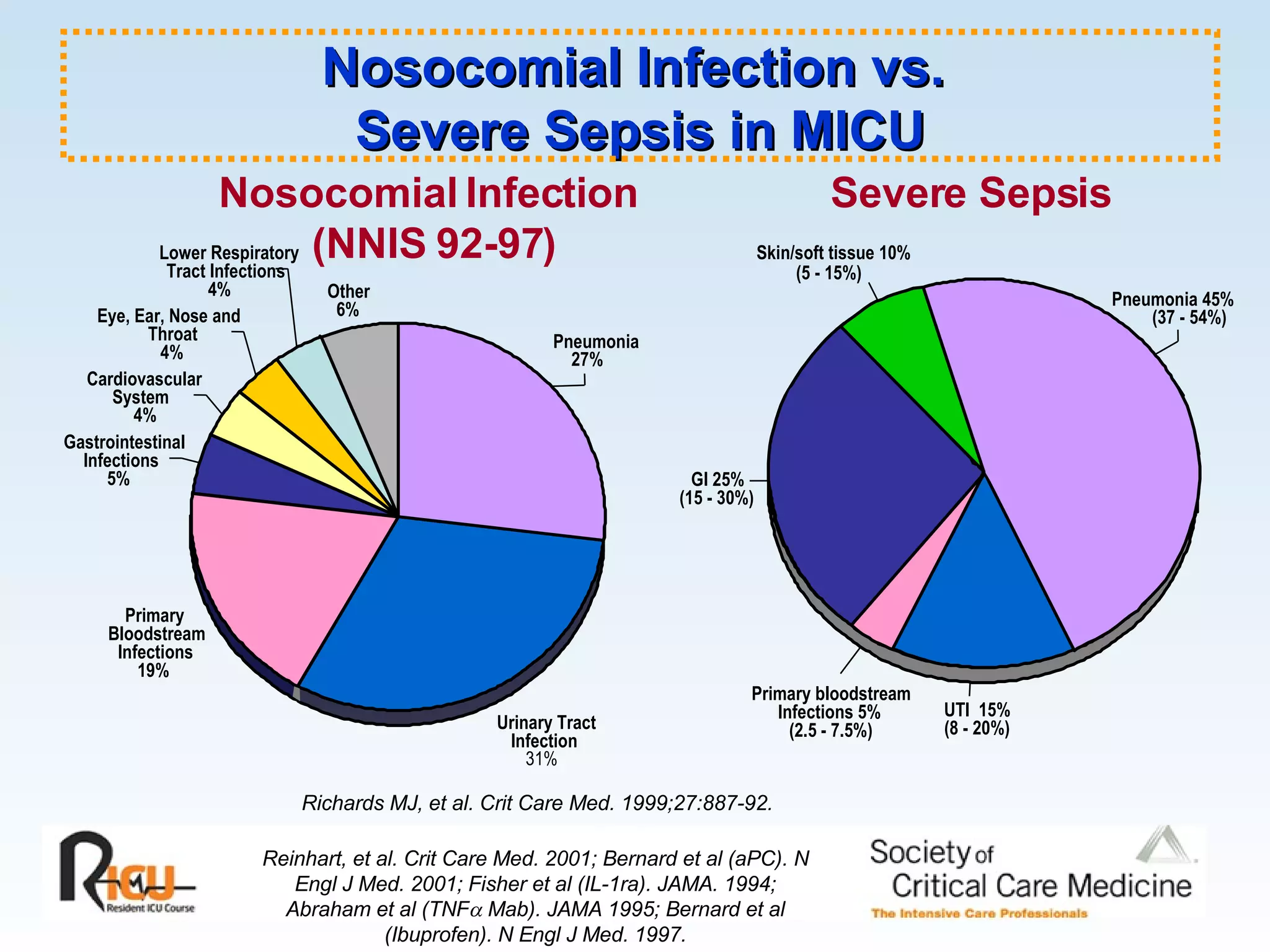
Nosocomial Infection vs. Severe Sepsis in MICU Reinhart, et al. Crit Care Med. 2001; Bernard et al (aPC). N Engl J Med. 2001; Fisher et al (IL-1ra). JAMA. 1994; Abraham et al (TNF Mab). JAMA 1995; Bernard et al (Ibuprofen). N Engl J Med. 1997. UTI 15% (8 - 20%) GI 25% (15 - 30%) Skin/soft tissue 10% (5 - 15%) Primary bloodstream Infections 5% (2.5 - 7.5%) Pneumonia 45% (37 - 54%) Richards MJ, et al. Crit Care Med. 1999;27:887-92. Urinary Tract Infection 31% Primary Bloodstream Infections 19% Gastrointestinal Infections 5% Cardiovascular System 4% Eye, Ear, Nose and Throat 4% Lower Respiratory Tract Infections 4% Other 6% Pneumonia 27% Nosocomial Infection (NNIS 92-97) Severe Sepsis
Pili Adapted fromYoung, et al. Ann Intern Med. 1977;86:456-71. Capsule (K antigen) Outer membrane Solid membrane (peptidoglycan) Flagellum (H antigen) LPS (endotoxin: O antigen) Oligosaccharide side chains Core polysaccharide Lipid A Inner cytoplasmic membrane Endotoxin (LPS): A Component of the Gram-negative Bacterial Cell Wall
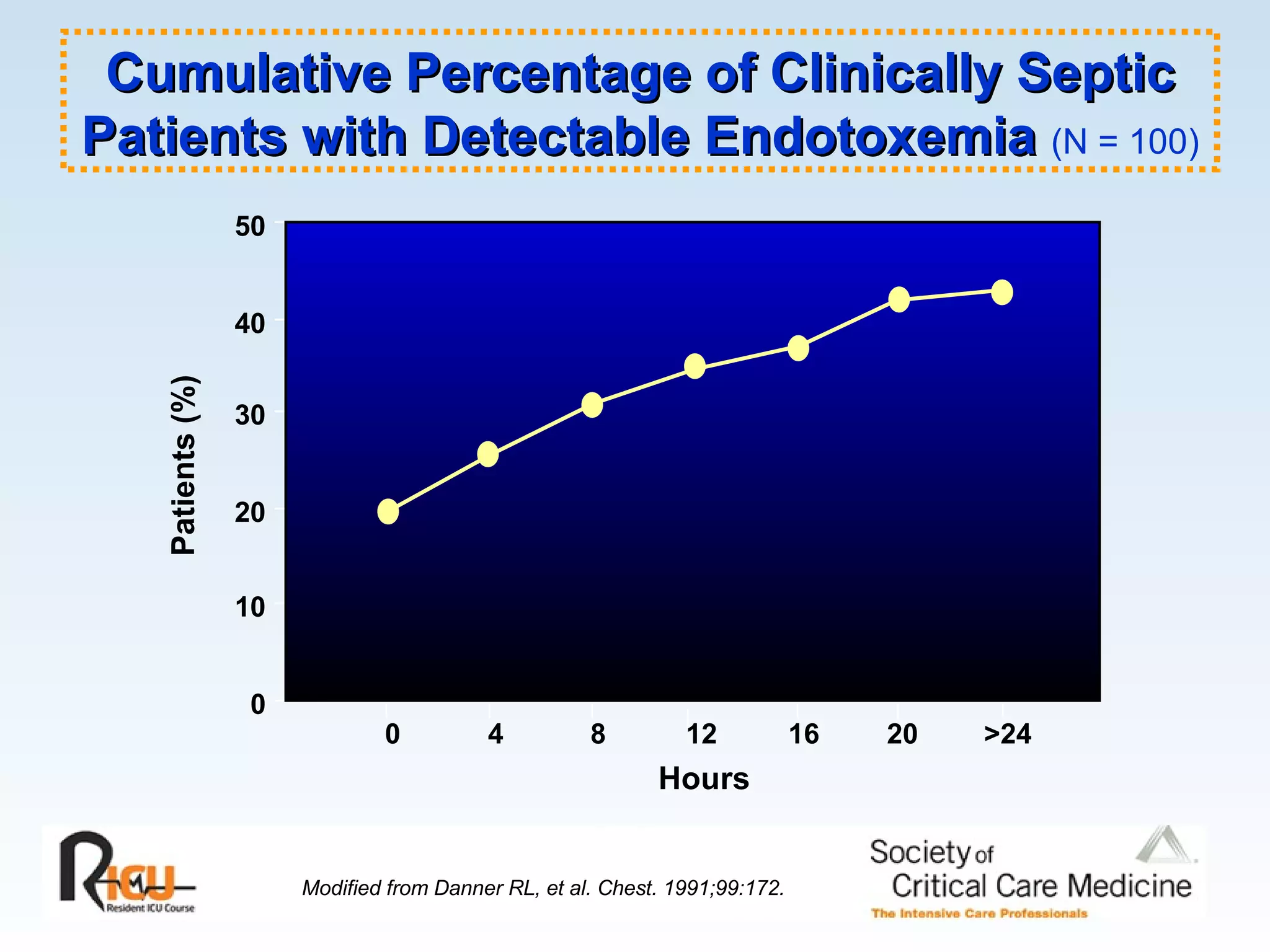
50 Patients (%)0 10 20 30 40 Modified from Danner RL, et al. Chest. 1991;99:172. Hours 0 4 8 12 16 20 >24 Cumulative Percentage of Clinically Septic Patients with Detectable Endotoxemia (N = 100)
22.
150,000 TNF units/mLserum 10 400 600 1,000 1,200 Waage A, Halstensen A, Espevick T. Lancet. 1987. Serum from patients who died Serum Concentrations in Survivors and Nonsurvivors of Septic Shock Serum from patients who survived Detection limit for TNF 100,000 1,400 1,000 200 Tumor Necrosis Factor (TNF)
Modern View ofthe Coagulation Cascade Steps in coagulation Coagulation cascade Initiation TF/VIIa Propagation VIIIa Thrombin activity Fibrinogen Fibrin IXa IX X Xa II Va IIa II indicates prothrombin; IIa, thrombin; IX, factor IX; IXa, activated factor IX; TF, tissue factor; Va, activated factor V; VIIa, activated factor VII; VIIIa, activated factor VIII; X, factor X; Xa, activated factor X. Weitz JI, et al. Chest. 2001.
28.
Coagulation in SepsisBernard GR, et al. New Engl J Med, 2001;344:699-709. Inflammatory Response to Infection Thrombotic Response to Infection Fibrinolytic Response to Infection Endothelium TAFI PAI-1 Suppressed fibrinolysis Neutrophil Monocyte IL-6 IL-1 TNF Bacterial, viral, fungal or parasitic infection/endotoxin Bacterial, viral, fungal or parasitic infection/endotoxin IL-6 Tissue Factor Tissue Factor COAGULATION CASCADE Factor Va Factor VIIIa THROMBIN Fibrin Fibrin clot
29.
30.
31.
Activation of Coagulationin Severe Sepsis Data from: Bernard et al. The Ibuprofen in Sepsis Trial (In Press). 0 20 40 60 80 100 Platelets PTT PT Any One Any Two All Three Protein C D-Dimers Percentage of Patients Markers of DIC
32.
Protein C LevelsDecrease Before the Clinical Diagnosis of Severe Sepsis Mesters et al. Crit Care Med. 2000;28:2209-16. 20 40 60 80 100 120 PC HEM WBC Fever 6 hr 12 hr 18 hr 24 hr 36 hr 48 hr 60 hr 72 hr PC Antigen (%) Severe Sepsis Patients Septic Shock Patients Average Time to Diagnose Severe Sepsis
33.
GTP cGMP BloodEndothelium Smooth Muscle GTP cGMP GC L-Arg O 2 L-citrulline GC NO . cNOS Platelets Nitric Oxide in the Vasculature
34.
GTP cGMP BloodEndothelium Smooth Muscle GTP cGMP GC L-Arg O 2 L-citrulline GC NO iNOS Platelets iNOS cNOS Endotoxin Cytokines NO Nitric Oxide in Sepsis
Septic Shock HemodynamicsCVP does not accurately estimate ventricular filling pressures in the critically ill. When PWP is appropriately elevated to 12 - 15 mm Hg with fluid resuscitation, 90% of patients with septic shock exhibit a hyperdynamic circulatory state. Hyperdynamic state persists to death
37.
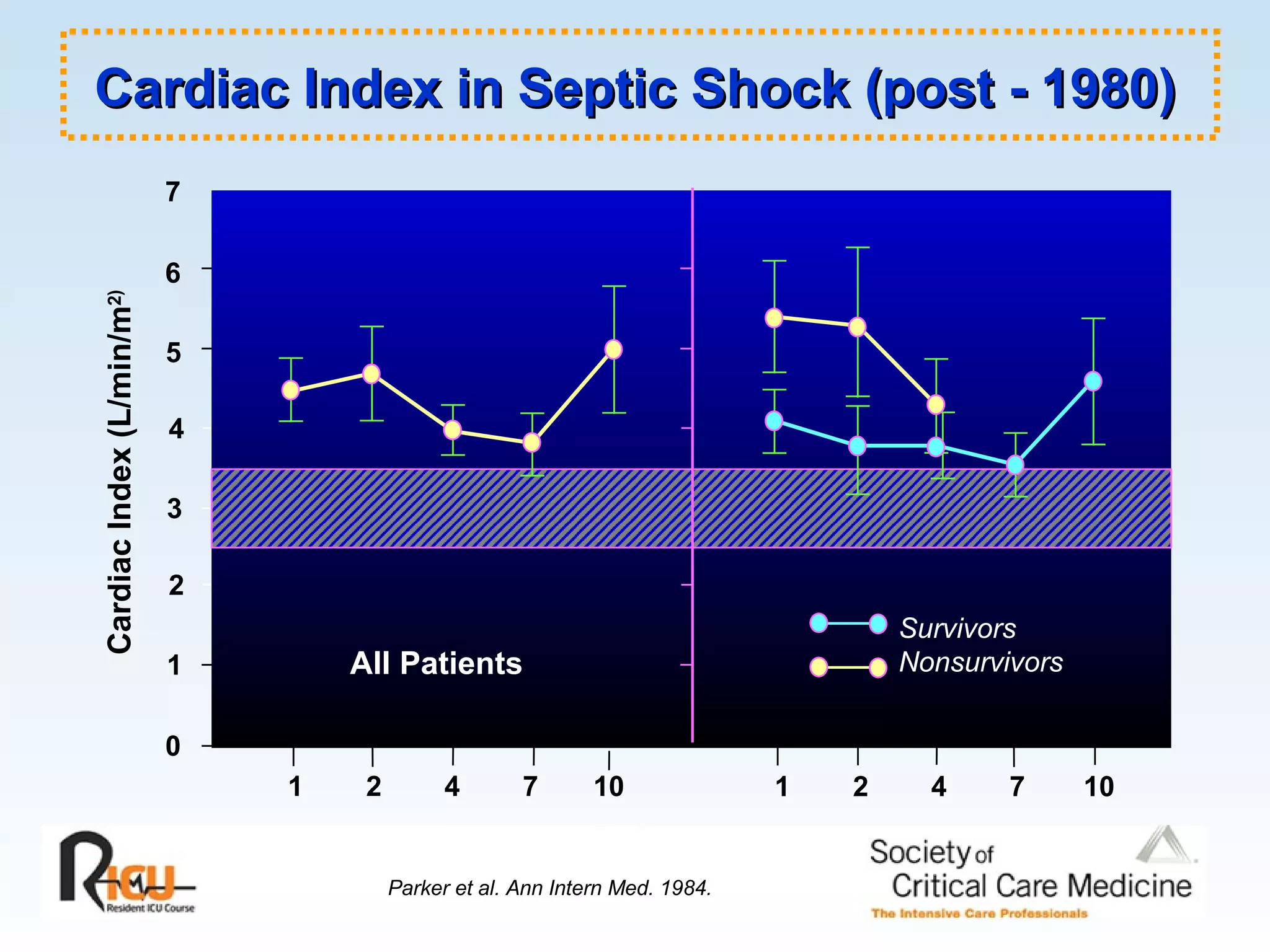
1 0 25 6 Cardiac Index (L/min/m 2) 3 4 1 2 4 7 10 1 2 4 7 10 Time (days) 7 Survivors Nonsurvivors All Patients Parker et al. Ann Intern Med. 1984. Cardiac Index in Septic Shock (post - 1980)
Metabolic Derangements inSepsis: Lactate, MVO 2 Micro-anatomic shunts (non-nutrient capillaries) Functional shunts (impaired micro-circulatory vasomotor control) Citric acid (Kreb’s) cycle defect with anaerobic glycolysis Aerobic glycolysis with lactate production
44.
References Annane D,Bellissant E, Cavaillon JM. Septic shock. Lancet . 2005;365:63-78. Aird WC. Vascular bed-specific hemostasis: role of endothelium in sepsis pathogenesis. Crit Care Med . 2001;29:S28-S34. Kumar A, Haery C, Parrillo JE. Myocardial dysfunction in septic shock. Crit Care Clin . 2000;16;251-287.