Downloaded 99 times
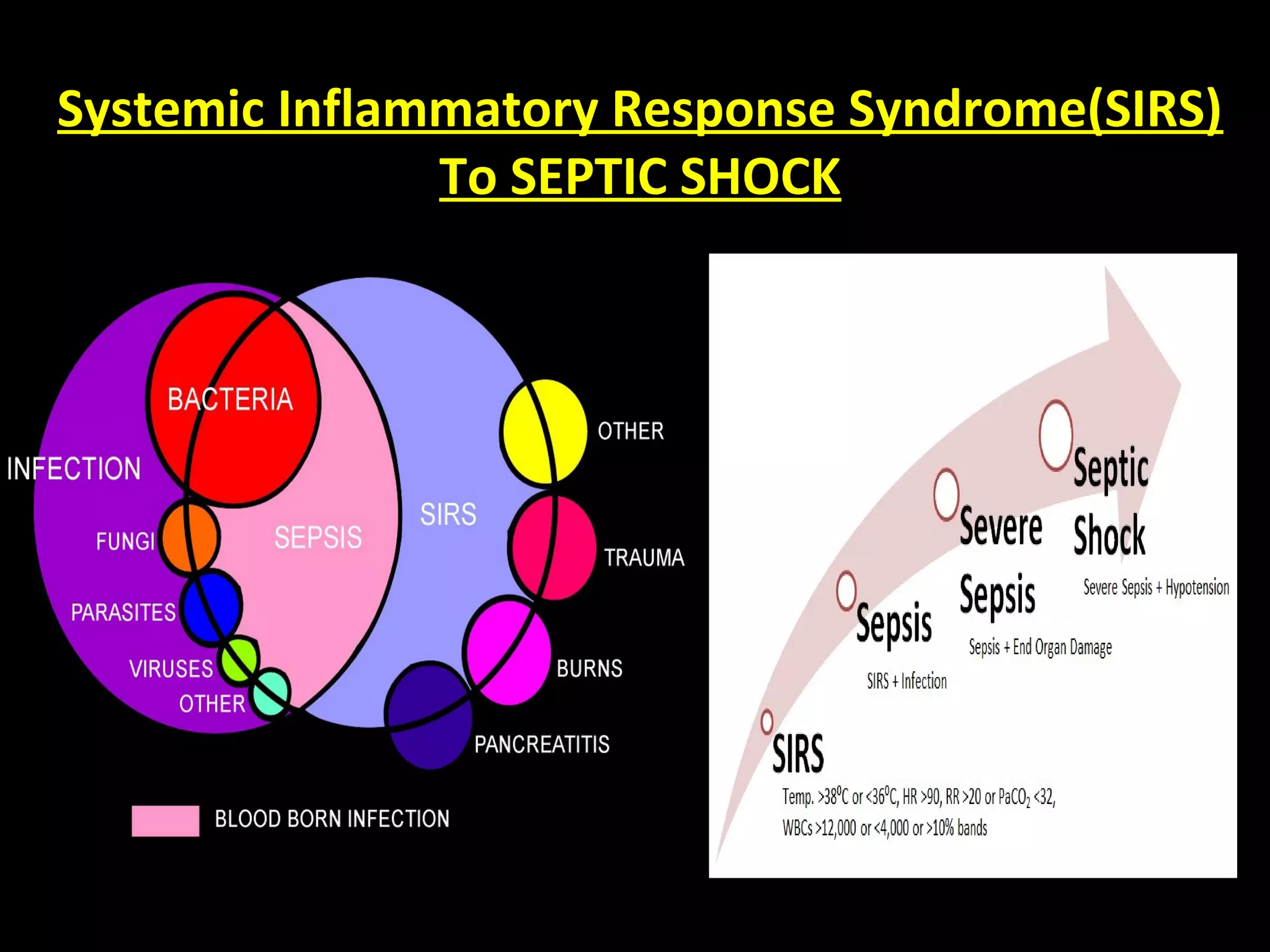
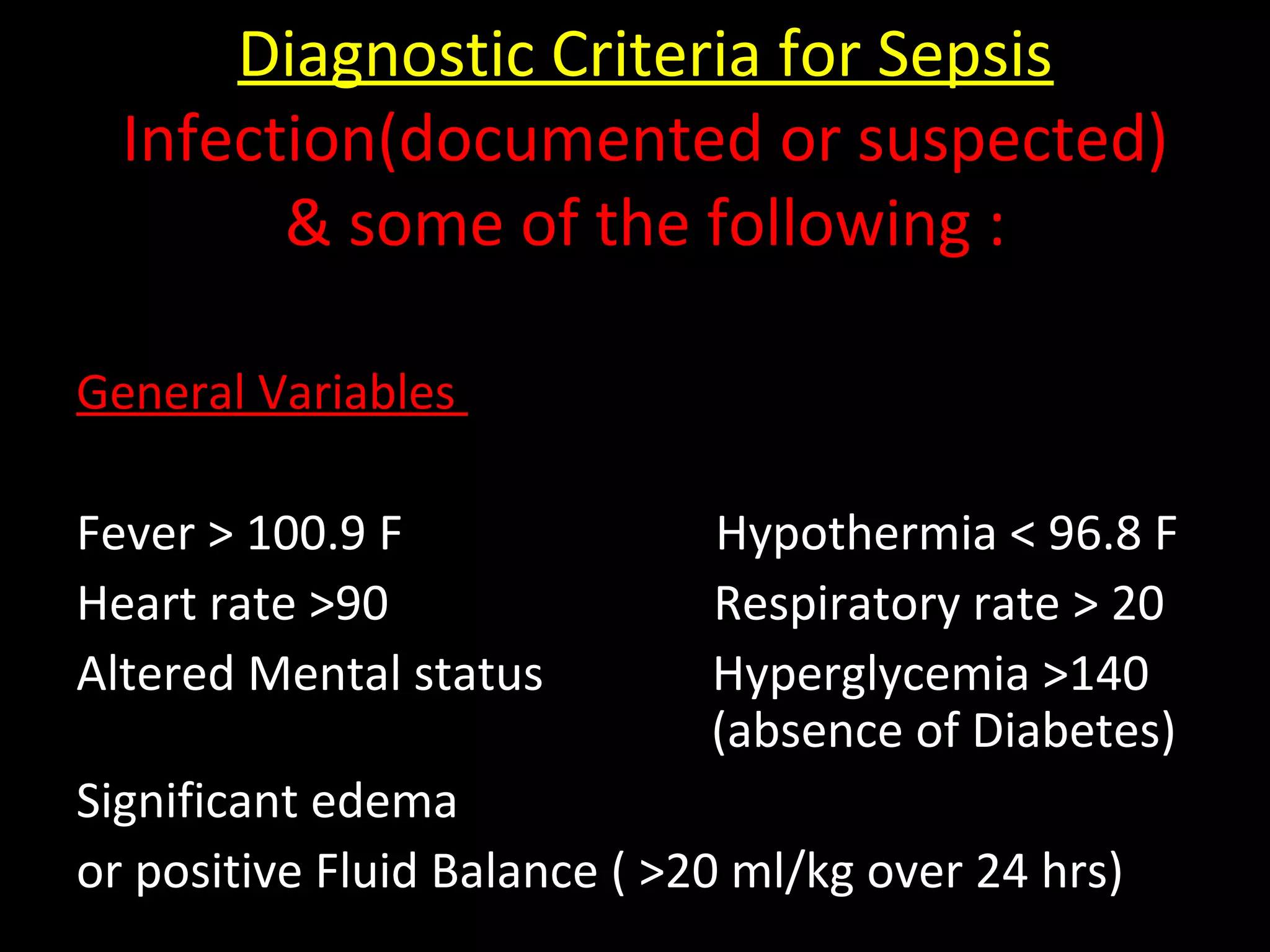
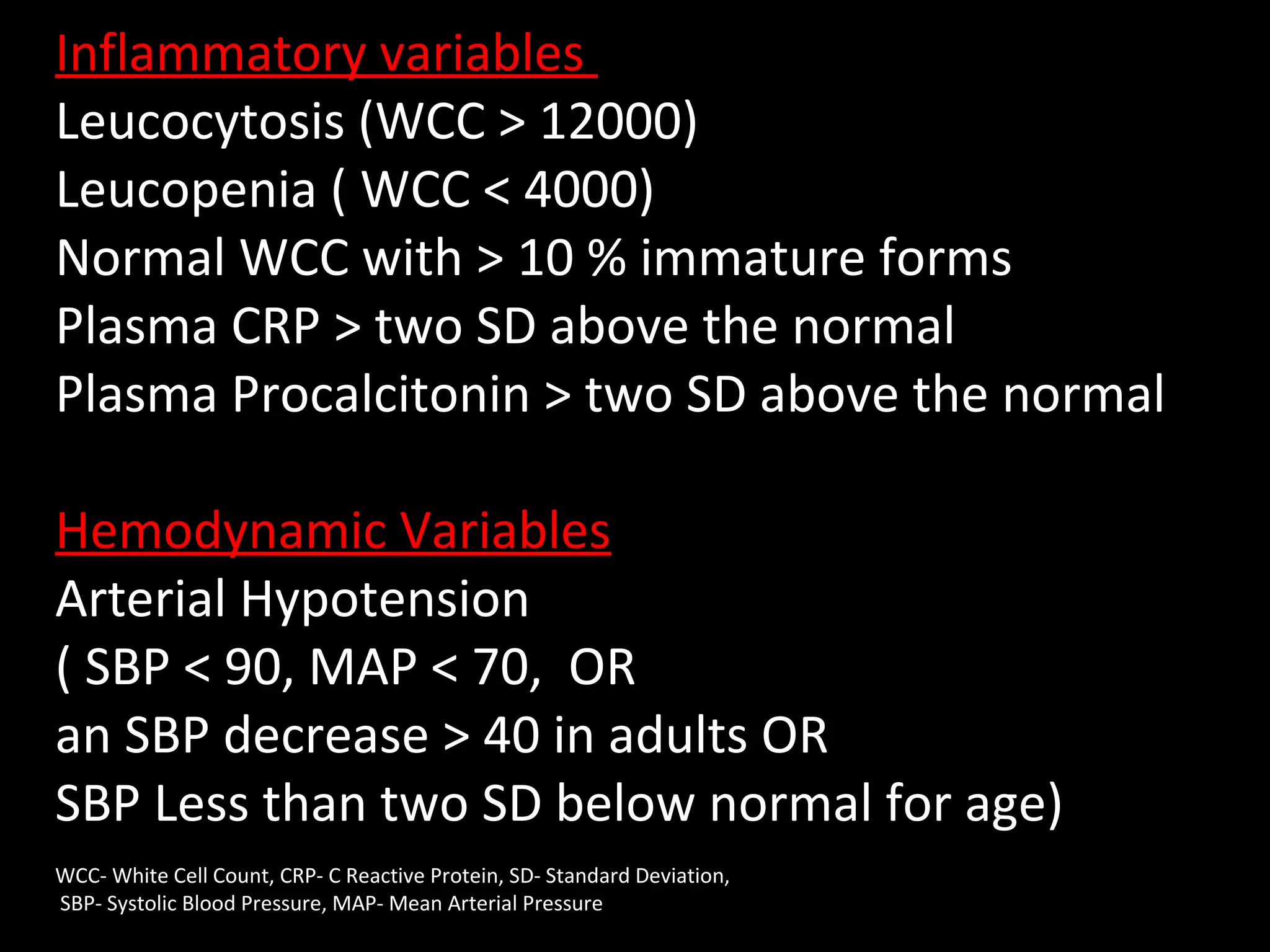
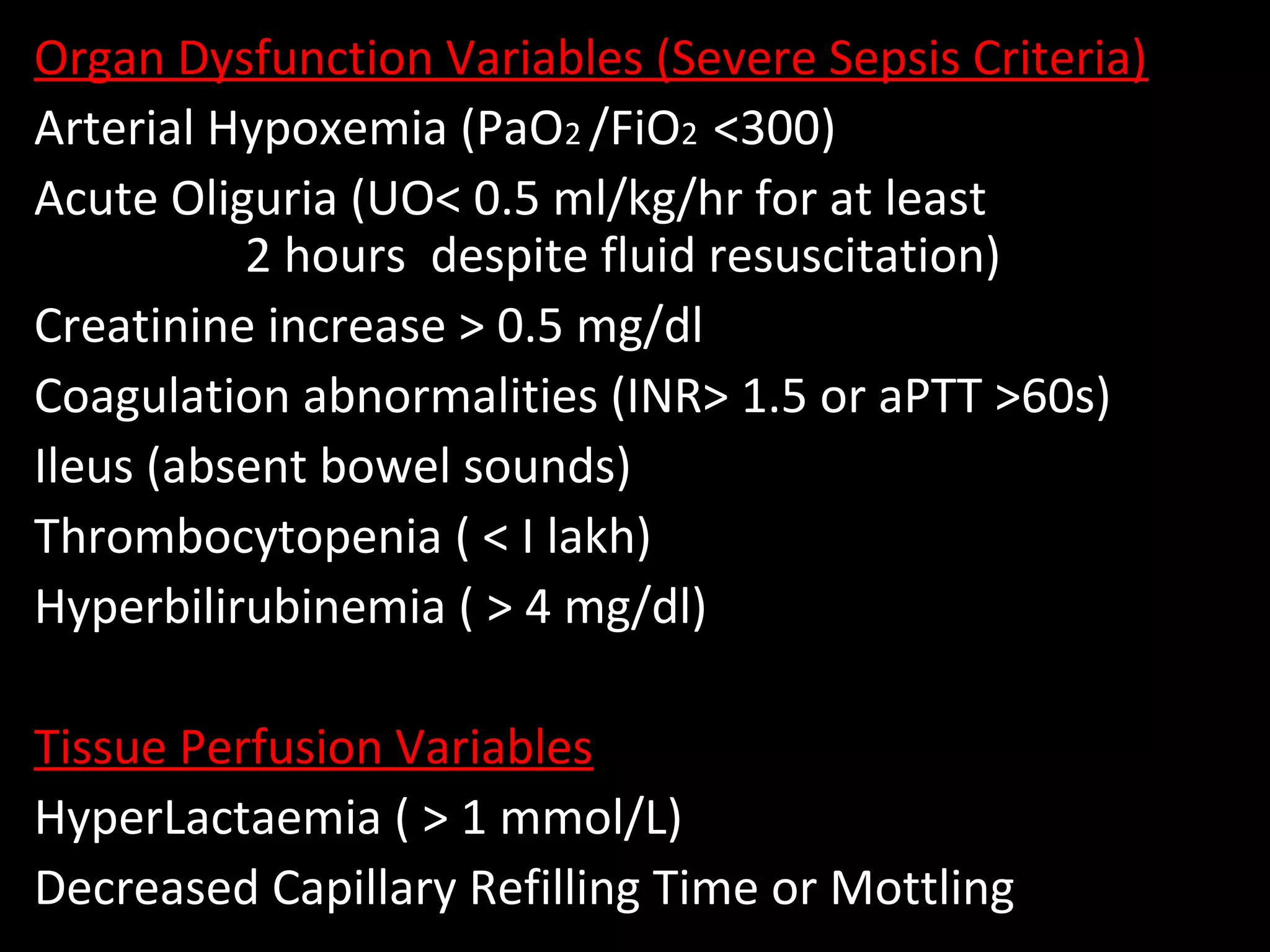
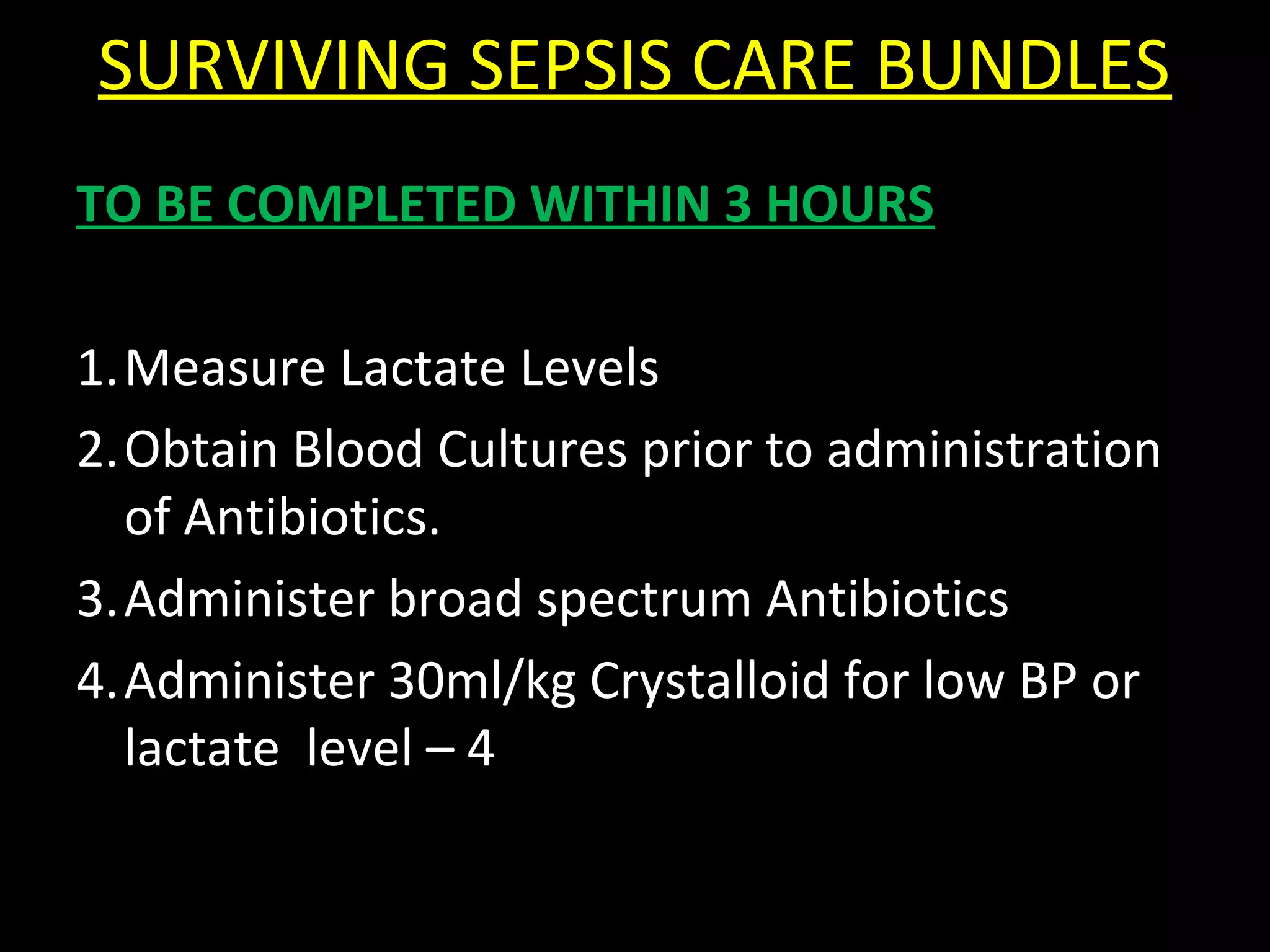
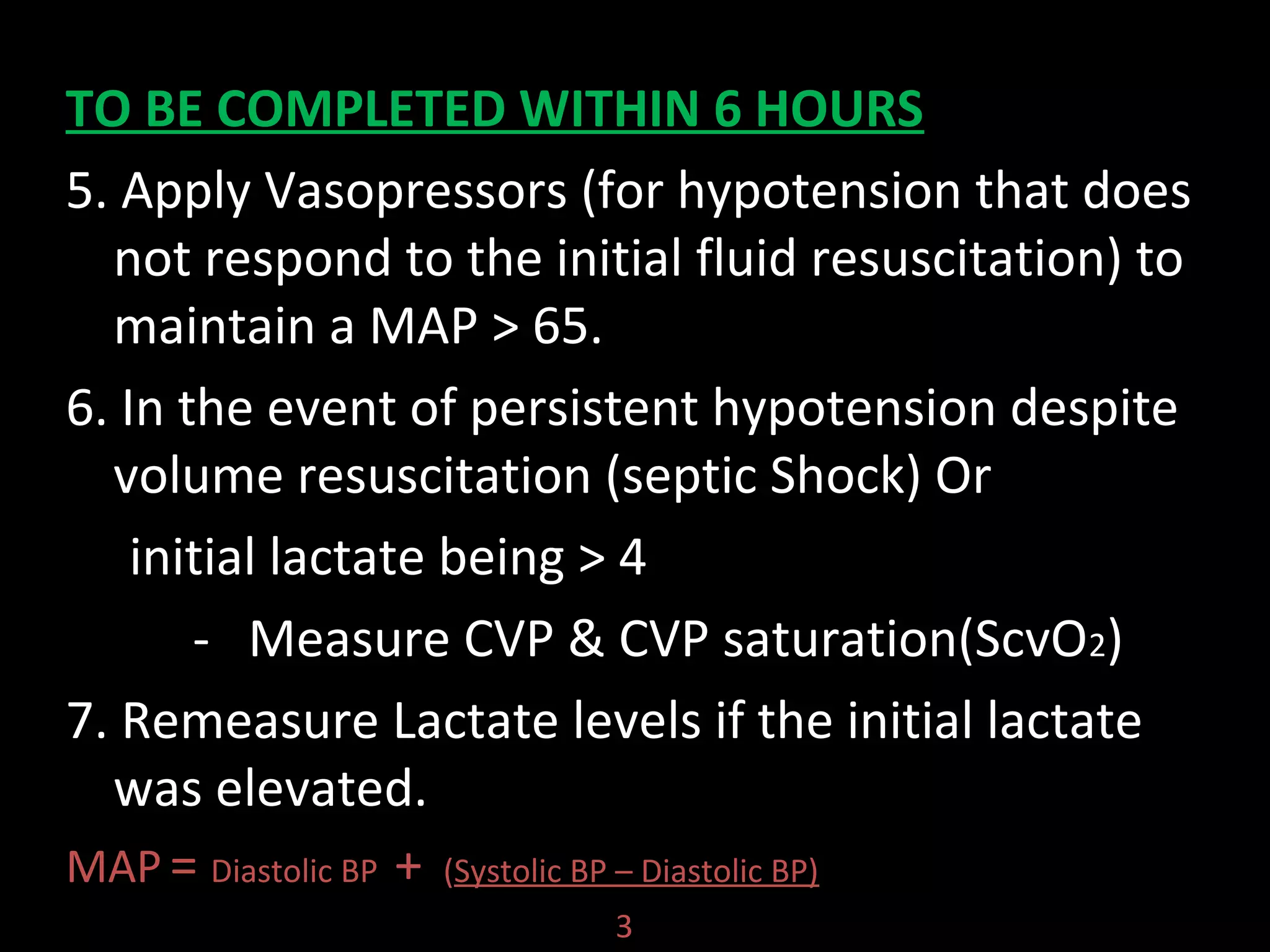
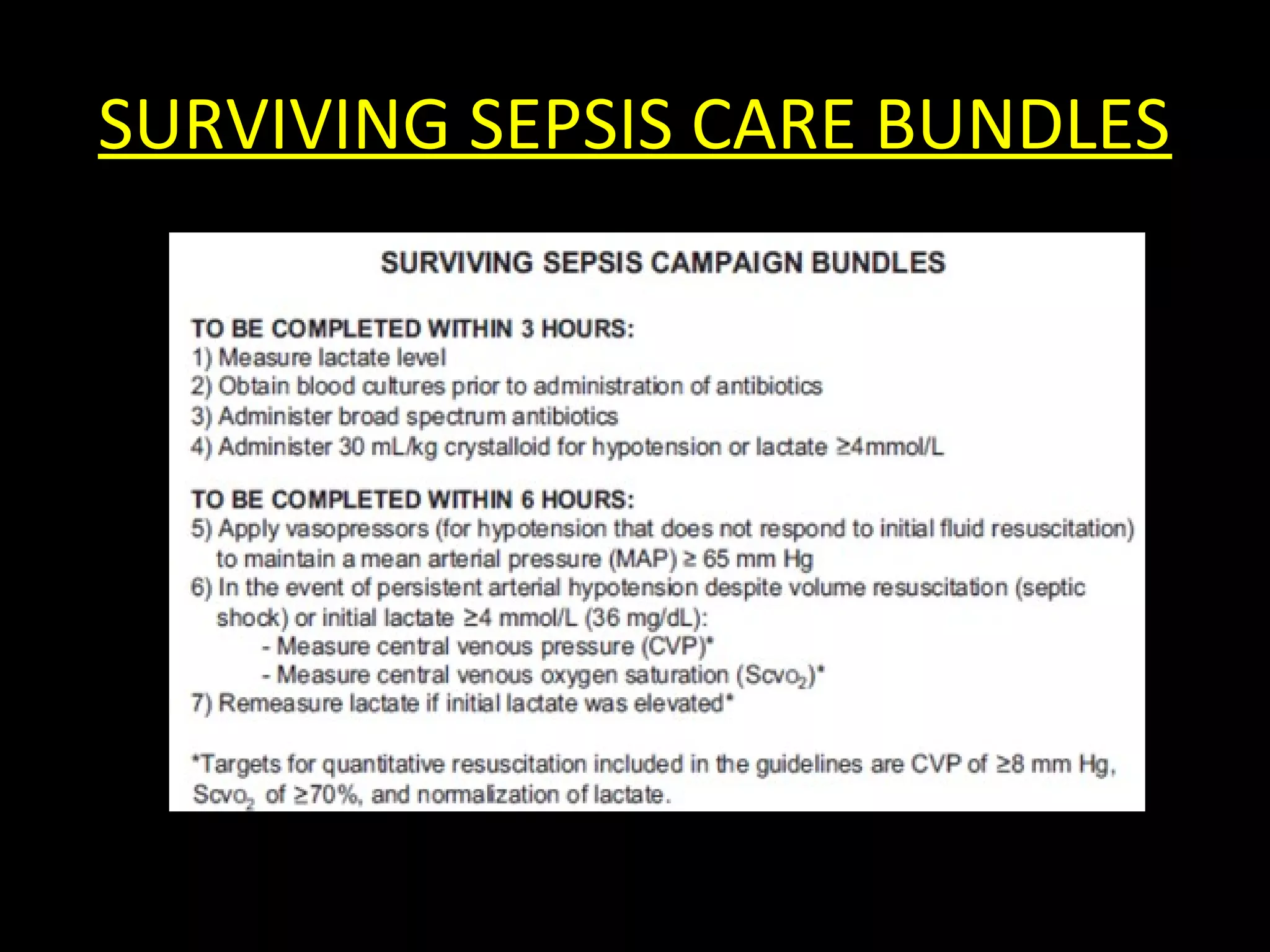











This document provides guidelines for the management of severe sepsis and septic shock according to the Surviving Sepsis Campaign. It outlines diagnostic criteria for sepsis, septic shock, and organ dysfunction. It also details bundles of care that should be completed within 3 and 6 hours of diagnosis, including measuring lactate levels, administering antibiotics and fluids, and applying vasopressors if needed. The guidelines provide recommendations on initial resuscitation, antibiotic therapy, source control, infection prevention, fluid therapy, vasopressors, corticosteroids, mechanical ventilation, and other supportive care measures for managing sepsis.



































































