Downloaded 1,993 times
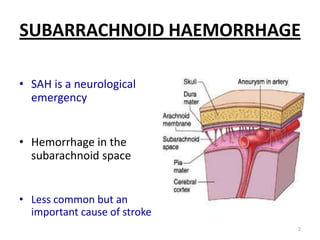
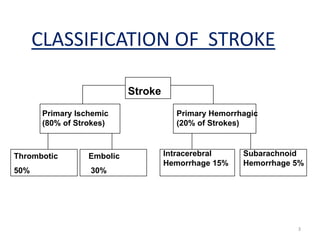


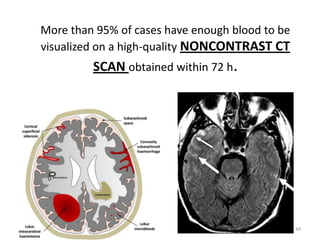
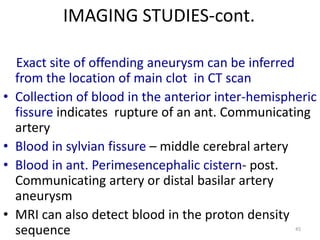
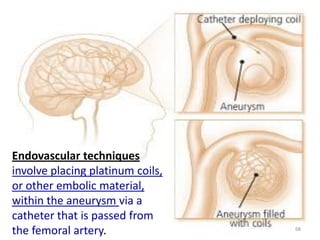


The document provides information on subarachnoid haemorrhage (SAH), including: - SAH is a neurological emergency caused by bleeding in the subarachnoid space, usually due to a ruptured saccular aneurysm. - Clinical manifestations include the sudden onset of the worst headache of one's life, neck stiffness, vomiting, focal neurological deficits, and loss of consciousness. - Investigations include non-contrast CT scan, which identifies the location and extent of subarachnoid blood in 95% of cases within 72 hours, and cerebral angiography to locate the aneurysm.