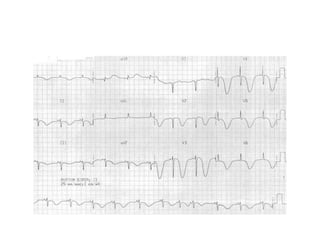
1. A 50-year-old female smoker with hypertension presented with sudden severe headache and brief loss of consciousness at work. She was found to have subarachnoid hemorrhage.
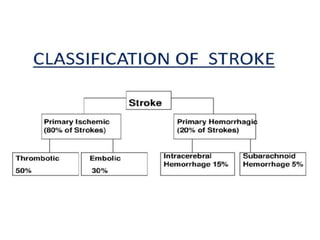
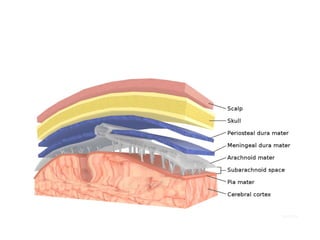
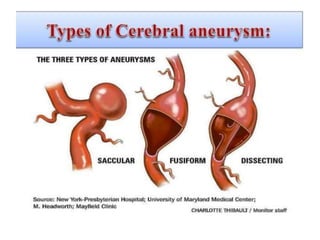
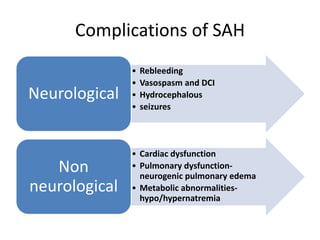
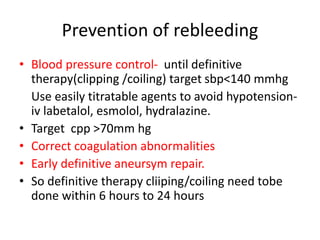
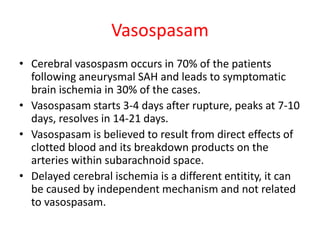
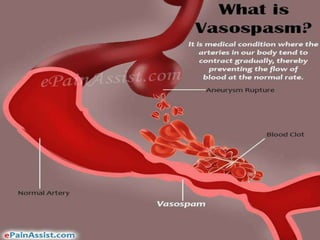
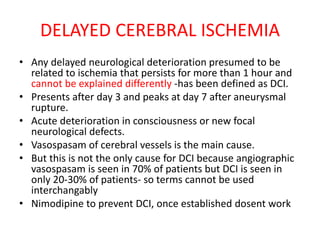
2. Subarachnoid hemorrhage is a neurological emergency caused by bleeding into the subarachnoid space, usually from a ruptured berry aneurysm. It requires rapid diagnosis and treatment to prevent rebleeding, vasospasm, and other complications.
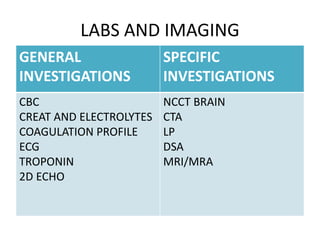
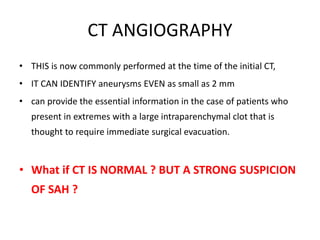
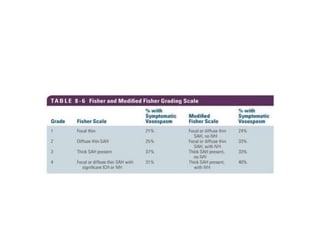
3. Diagnostic tests included a non-contrast CT, which was positive, as well as a CTA and lumbar puncture to confirm the diagnosis and identify the source of bleeding. The patient was treated supportively in the ICU to control






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)